Impedance
Opposition tothe flow of sound energy is called as
IMPEDANCE
Opposition of Admittance (Ease with which energy flow)
( mho)
Impedance of the medium : Complex mixture of 3
parameters- stiffness, mass, friction
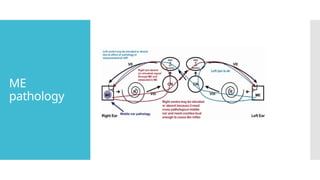
Middle ear (ME) act as the impedance matching device
All ME pathologies alter this impedance , result in lesser
sound energy being transmitted to the cochlea
3.
Impedance
matching by
ME system
Area of tympanic membrane relative to oval window
(Areal Ratio)
The lever action of ossicles
Mobility of TM
4.
Areal Ratio
Totalarea of TM 90mm2
Functional area of TM is 55mm2
Area of Stapes footplate is 3.2mm2
Effective areal ratio is 17:1
Thus by focusing sound pressure from large area of TM to
small area of oval window, effectiveness of energy
transfer between air to fluid of cochlea is increased.
5.
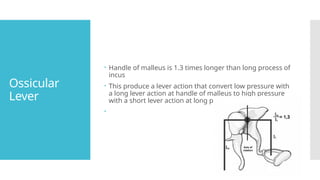
Ossicular
Lever
Handle ofmalleus is 1.3 times longer than long process of
incus
This produce a lever action that convert low pressure with
a long lever action at handle of malleus to high pressure
with a short lever action at long process of incus
6.
Mobility of
TM
Centralpart of TM has limited mobility compared to
periphery.
Result in transfer of most of energy to ossicles.
Act as Curved membrane effect.
7.
• Objective Test
•Uses of Impedance Audiometry
Objective differentiation between CHL and SNHL
Measurement of middle ear pressure and evaluation of Eustachian tube function
• Impedance Audiometry include:
1. Tympanometry
2. Stapedial reflex
3. Eustachian Tube Function Test
8.
Principle of
Tympanometr
y
Soundstrikes the TM – some energy is absorbed and
some energy reflected.
Stiffer TM – reflects more energy than compliant one.
By changing the pressure in a sealed EAC and measuring
the reflected sound energy – possible to find the
compliance/stiffness of tympano ossicular system.
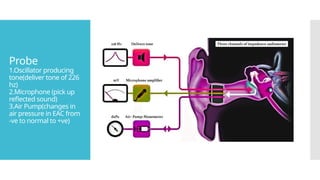
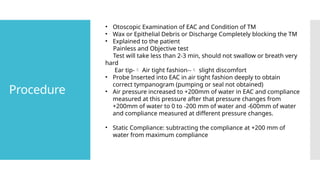
Procedure
• Otoscopic Examinationof EAC and Condition of TM
• Wax or Epithelial Debris or Discharge Completely blocking the TM
• Explained to the patient
Painless and Objective test
Test will take less than 2-3 min, should not swallow or breath very
hard
Ear tip- Air tight fashion-- slight discomfort
• Probe Inserted into EAC in air tight fashion deeply to obtain
correct tympanogram (pumping or seal not obtained)
• Air pressure increased to +200mm of water in EAC and compliance
measured at this pressure after that pressure changes from
+200mm of water to 0 to -200 mm of water and -600mm of water
and compliance measured at different pressure changes.
• Static Compliance: subtracting the compliance at +200 mm of
water from maximum compliance
12.
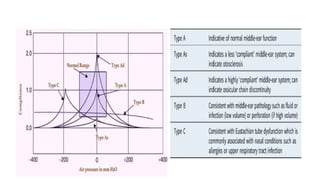
• Result ofTympanometry Test displayed graphically with compliance on Y-Axis and Air
Pressure on X-Axis known as Tympanogram.
• Air pressure measured millimeter of water pressure unit
• Compliance measured in cubic centimeter or milliliter
• Compliance of TM – Normal range of static compliance –is -0.35 to 1.40 ml
• ME pressure- Normal pressure is -50 to +50 mm of water
14.
Compliance
With Increased
Compliance
1.Ossi.chain
Discontinuity
2. Scarred TM
3. Large TM
4. Post.Stapedecto
my ear
• Decreased
Compliance
1. Otosclerosis
2. Adhesive Secretory
OM
3. Glomus jugulare
4. Fixed Malleus
syndrome
• Normal Compliance
1. ET obstruction
without secretory
changes in ME
15.
ME Pressure
• NegativeME
Pressure
1. Blocked ET
2. OM with
Effusion
• Normal ME
Pressure
1. Otosclerosis
2. Ossi.Chain
discontinuity
3. Scarred TM
4. Fixed Mlleus
syndrome
• Positive ME
Pressure
1. Early AOM
• Absence of
any pressure
peak
1. Adhesive
OM
2. Perforated
TM
3. Artifact(Bloc
ked probe
tip)
4. Patent
grommet in
TM
5. Wax
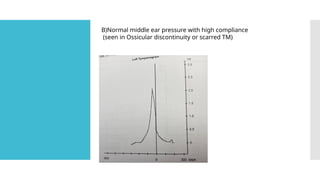
B)Normal middle earpressure with high compliance
(seen in Ossicular discontinuity or scarred TM)
18.
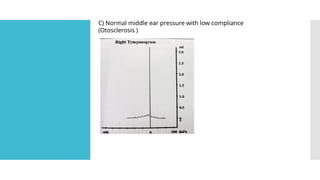
C) Normal middleear pressure with low compliance
(Otosclerosis )
19.
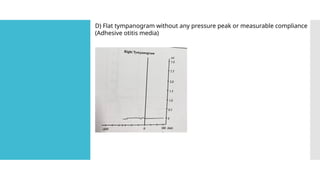
D) Flat tympanogramwithout any pressure peak or measurable compliance
(Adhesive otitis media)
20.
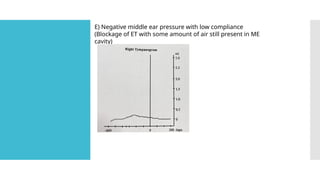
E) Negative middleear pressure with low compliance
(Blockage of ET with some amount of air still present in ME
cavity)
21.
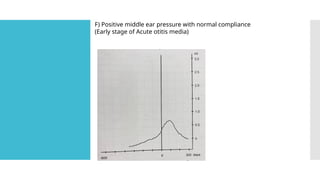
F) Positive middleear pressure with normal compliance
(Early stage of Acute otitis media)
22.
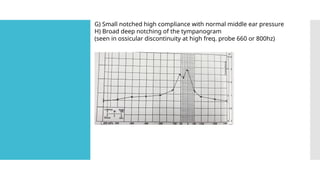
G) Small notchedhigh compliance with normal middle ear pressure
H) Broad deep notching of the tympanogram
(seen in ossicular discontinuity at high freq. probe 660 or 800hz)
23.
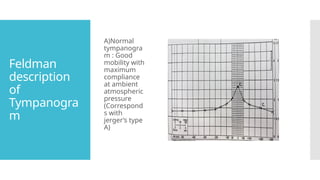
Feldman
description
of
Tympanogra
m
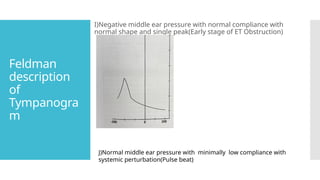
I)Negative middle earpressure with normal compliance with
normal shape and single peak(Early stage of ET Obstruction)
J)Normal middle ear pressure with minimally low compliance with
systemic perturbation(Pulse beat)
24.
Fallacies of
Tympanometr
y
• Itis Objective test , it is not without errors
• Some conditions where tympanogram does not give true picture of
ME pathology
• Mainly when there is two or more ME pathology are
present ,compliance is representative of the more lateral ME
pathology
• Examples
1. A patient with otosclerosis and Eustachian tube dysfunction (from a
cold) may show negative middle ear pressure and low compliance
on tympanometry, mimicking otitis media with effusion. This can
lead to a misdiagnosis.
2. A patient with a scarred tympanic membrane but developing
otosclerosis may present a Type Ad tympanogram with high
compliance. This pattern usually suggests ossicular chain
discontinuity.
25.
Fallacies of
Tympanometr
y
3. Apatient with tympanic membrane thickening but otherwise normal
hearing, this patient will present with As type of graph which is particular
for Otosclerosis. If this patient may develop tubal dysfunction from a cold,
causing a negative pressure, low compliance tympanogram. This can
falsely suggest OME, even when no middle ear fluid is present.
26.
EUSTACHIAN
TUBE
FUNCTION
TEST
Physiological functionof ET:
1) Maintenance of equality of air pressure between the
middle ear and the ambient atmosphere(ventilatory
function)
2) Drainage of the mucus from the ear to the nasopharynx
(mucociliary clearance function)
27.
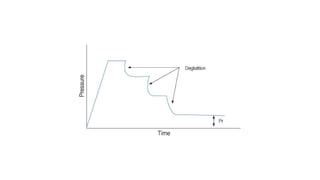
William’s Test
Testof Tubal Function with intact TM
Measure the middle ear pressure in three condition 1)
resting phase 2) while patient swallows 3) finally after
performing Valsalva.
Normally at resting phase middle ear pressure is at or
near environmental atmospheric pressure, become
negative while swallows and become positive after
Valsalva
Any deviation as abnormal
Partially impaired ET function : middle ear pressure
become negative at swallows but remain negative after
Valsalva
Grossly impaired ET function : Middle ear pressure does
not change at all during swallows or valsalva
29.
Toynbee’s
Test
Done inpatient with Perforated TM
Artificially increased or decreased pressure in the middle ear and
then record the change of middle ear pressure each time patient
swallows
Carried out for fixed duration of time (min.40 sec to max. 160 sec)
Air pressure at middle ear end of ET is changed either +250 or -250
mm of water.
Ask patient to swallow repeatedly- pressure will be partially
neutralized with each swallow
Normally pressure should be totally neutralize after 3 to 4 swallow
If some residual pressure persist even after 5 swallow – partially
Can not be neutralize at all by repeated swallowing –grossly.
Principle
Loud soundreach the ear
Stapedius and tensor tympani muscle contract reflexly
Pull the stapes outward and upward, tympanic
membrane inward
Change the impedance of middle ear system
Changes are monitored and analyzed by electroacoustic
bridge and result displayed accordingly
34.
Acoustic
Reflex
Threshold
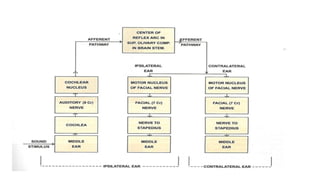
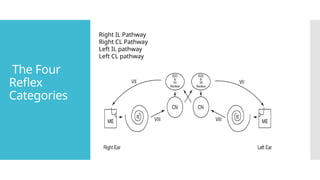
The signal entersthe right ear, travels through the outer, middle (ME),
and inner ear (IE), along the VIII nerve to the brainstem. When the
signal reaches the brainstem, the signal arrives first at the cochlear
nucleus (CN). From here, the signal travels to both right and left
superior olivary complexes and both right and left facial nerve (VII)
nuclei. The signal is sent from both facial nerve nuclei to both facial (VII)
nerves, which results in a contraction of both stapedius muscles. Thus,
both stapes bones are pulled outward and downward, in a direction
away from the inner ear. This action makes it harder for energy to travel
through the middle ear (increase in impedance/decrease in
admittance). The lowest intensity level at which this contraction is
measurable is the ART.
35.
Clinical
significance
of Stapedial
Reflex
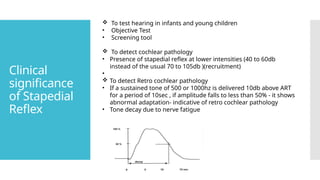
Totest hearing in infants and young children
• Objective Test
• Screening tool
To detect cochlear pathology
• Presence of stapedial reflex at lower intensities (40 to 60db
instead of the usual 70 to 105db )(recruitment)
•
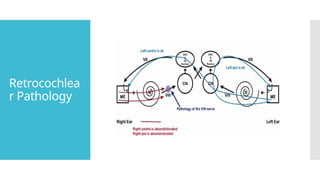
To detect Retro cochlear pathology
• If a sustained tone of 500 or 1000hz is delivered 10db above ART
for a period of 10sec , if amplitude falls to less than 50% - it shows
abnormal adaptation- indicative of retro cochlear pathology
• Tone decay due to nerve fatigue
36.
Clinical
significance
of Stapedial
Reflex
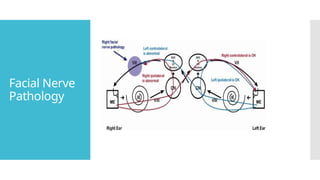
Lesionof facial nerve
• Stapedial reflex absent( if injury is before the origin of the nerve of
stapedius)
• Stapedial Reflex present ( if injury is beyond the origin of the nerve
of stapedius)
To find malingerers
• Doesn’t give response on PTA, shows positive stapedial reflex
37.
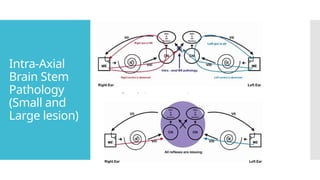
Afferent
pathway
IL middleear disease causing moderate to severe CHL
Lesion in IL cochlea or 8th
cranial nerve (causing severe SNHL)
Lesion in IL cochlear nucleus or superior olivary complex
38.
Efferent
pathway
Lesion infacial nerve nucleus at brain stem level
Facial nerve paralysis before proximal to origin of nerve
of stapedius
Disease of Stapedius muscle like myasthenia gravis