Downloaded 383 times

![Conventions used in the Tabular list
Parentheses ( )
• used to enclose supplementary words, which may follow
a diagnostic term without affecting the code number
For example, in I10, the inclusion term, ‘Hypertension
(arterial)(benign)(essential)(malignant) (primary)(systemic)’,
implies that I10 is the code number
• used to enclose the code to which an exclusion term refers.
Square brackets [ ]
• for enclosing synonyms, alternative words or explanatory
phrases; e.g.
A30 Leprosy [Hansen disease]
• for referring to previous notes](https://image.slidesharecdn.com/icd10-160923053430/85/Icd-10-41-320.jpg)
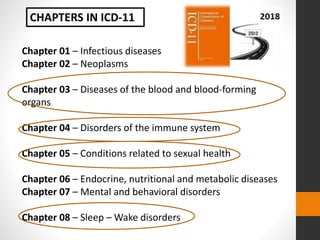
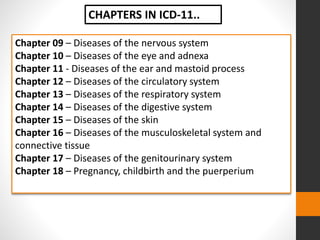
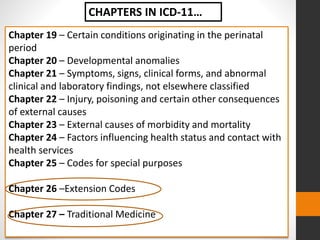
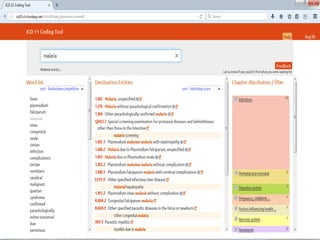


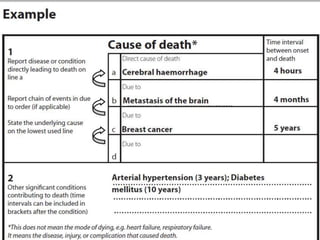
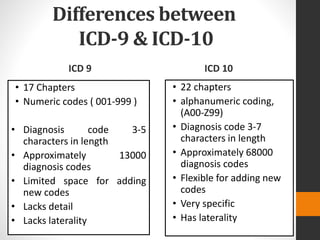
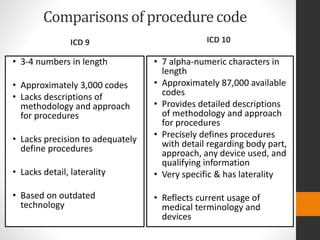
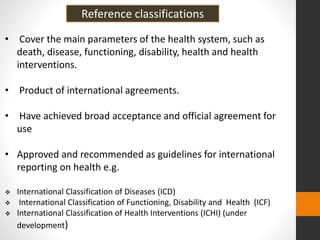
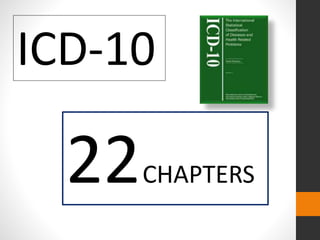
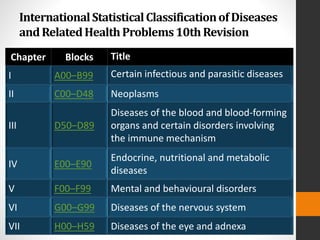
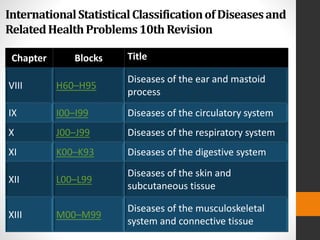
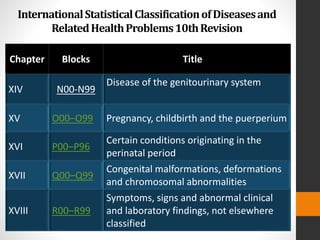
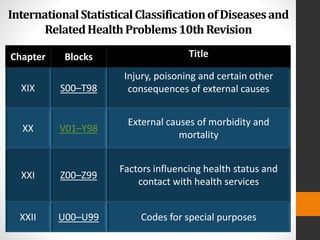
The document provides an overview of the International Classification of Diseases (ICD) including: 1) A brief history of disease classification systems leading to the development of the ICD by the World Health Organization. 2) An explanation that the ICD-10 is the current international standard for morbidity and mortality statistics and coding of diseases and health problems. 3) A summary of the structure of ICD-10 including its 3 volumes, 22 chapters and alphanumeric coding system.



































































