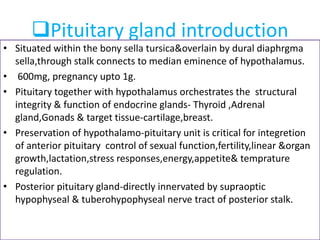
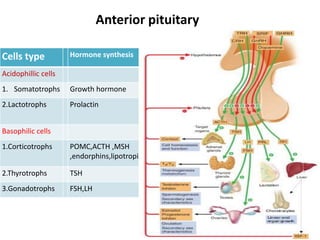
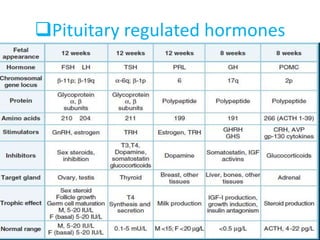
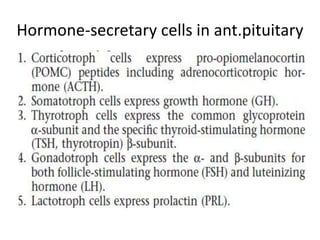
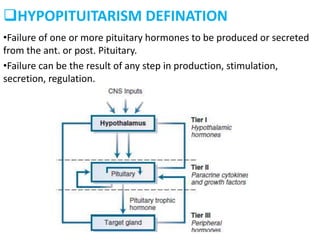
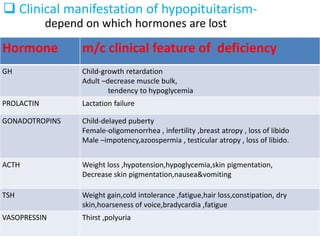
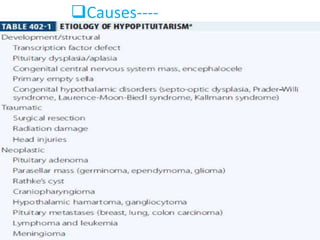
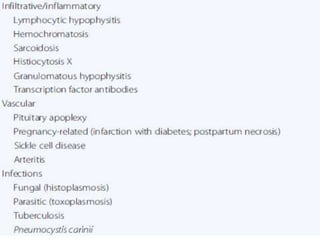
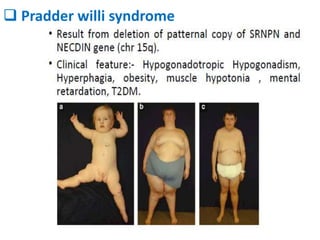
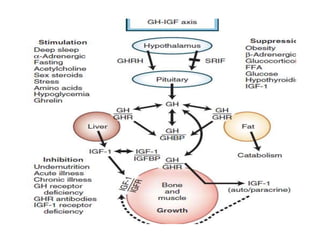
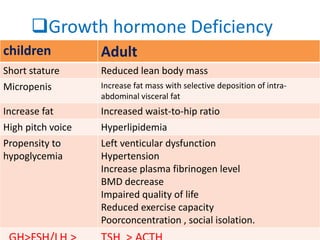
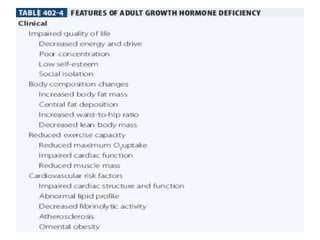
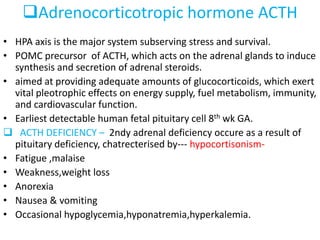
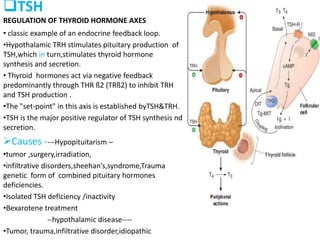
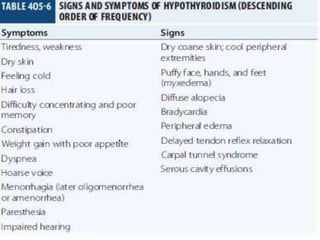
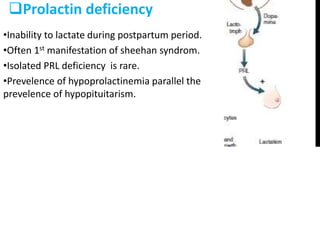
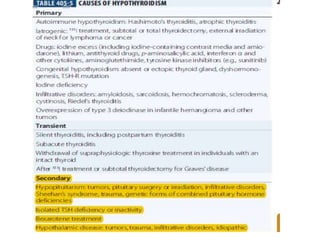
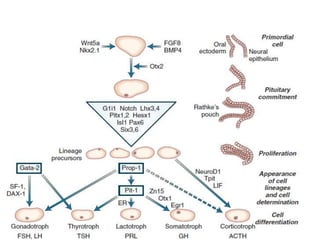
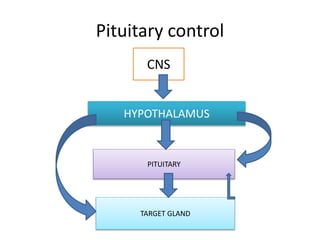
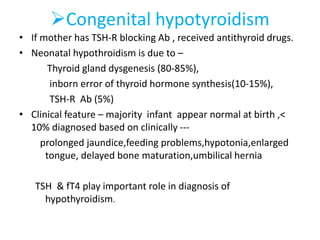
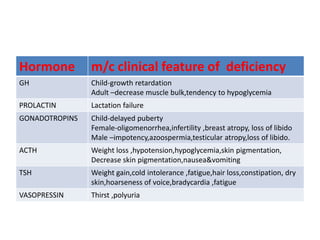
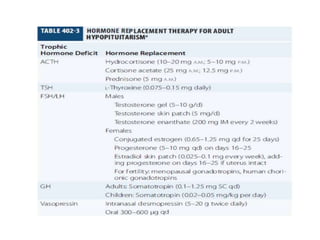
Hypopituitarism is a condition where the pituitary gland fails to produce or secrete one or more hormones. This can result from defects in pituitary development, genetic conditions, tumors, trauma, or other causes. Deficiencies in specific pituitary hormones lead to distinct clinical effects, such as short stature from growth hormone deficiency, infertility from gonadotropin deficiency, or weight gain and fatigue from TSH deficiency. The document provides details on the causes, clinical presentations, and hormone deficiencies associated with hypopituitarism.