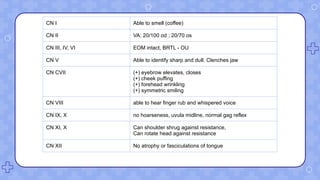
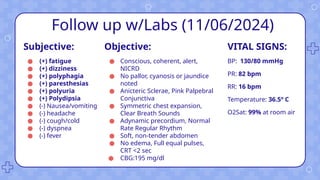
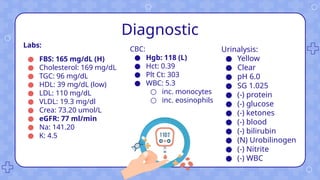
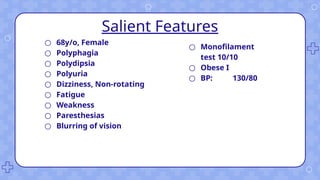
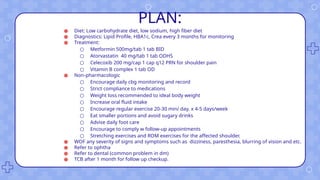
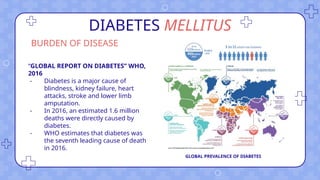
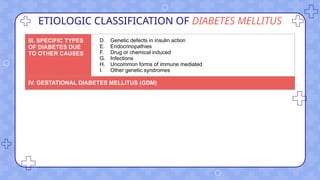
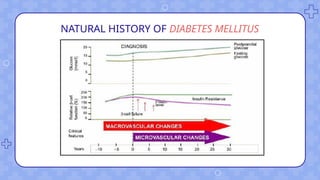
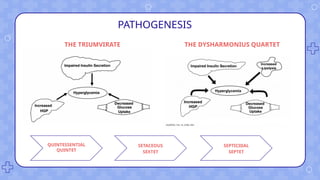
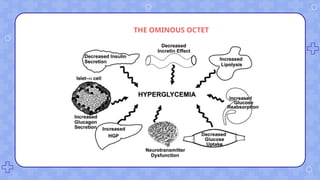
The document presents a detailed medical case of a 68-year-old Filipino female with type 2 diabetes, showing symptoms like dizziness, fatigue, and polyuria. It outlines her medical history, physical examination findings, diagnostic tests, and a treatment plan involving medication and lifestyle modifications. The case also discusses the prevalence and classification of diabetes mellitus, emphasizing the importance of early detection and management.