Downloaded 214 times



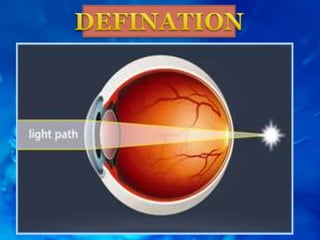
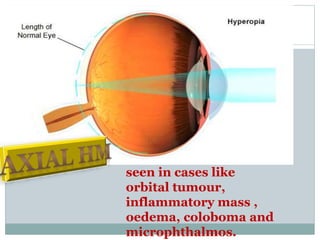
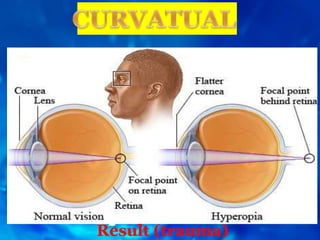


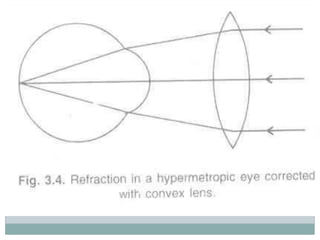
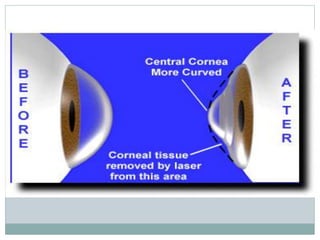


This document summarizes hyperopia (farsightedness), including its etiology, clinical types, latent and manifest presentations, symptoms, signs, and treatment options. The main points are: Hyperopia is caused by an eyeball that is too short or a cornea that is too flat. It can be developmental, pathological, or functional in nature. Symptoms include tiredness, headaches, and blurred distance vision. Examination may reveal a small eye size. Treatment includes glasses, contact lenses, or refractive surgery to bring light to a focus on the retina.















































