Hyperlipidemia
abnormally elevated levelsof any or all lipids
and/or lipoproteins in the blood but Plasma
cholesterol and triglyceride are clinically
important because they are major modifiable
risk factors for cardiovascular disease, whilst
severe hypertriglyceridaemia also predisposes
to acute pancreatitis
.
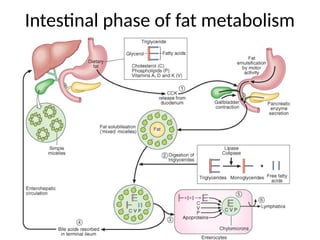
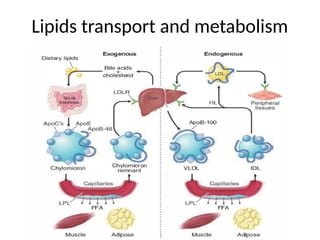
Fat transport andmetabolisim
The term 'lipid' refers to substances (including free cholesterol ,
cholesterol ester , phospholipid , triglyceride ) with poor water
solubility therefore to be transport and metabolize should combined
with apolipoproteins to form spherical or disk-shaped lipoprotein
which consist of a hydrophobic core and a hydrophilic coat The
structure of apolipoproteins enables them to act as cell receptor
ligands (by which lipoprotein can attach to the cells ) . Thus, variation
apolipoproteins composition results in the formation of distinct classes
of lipoproteins with different metabolic functions
.
5.
Therefore according todifferent type of apolipoproteins and lipids
those they contain . lipoproteins can subdivided to
HDL LDL IDL VLDL Chylomicron R
.
Apo A-1 ApoB100 ApoB100 ApoB100 ApoB48
5
1
CONCLUSION AND CLINICALIMPORTANCE
●
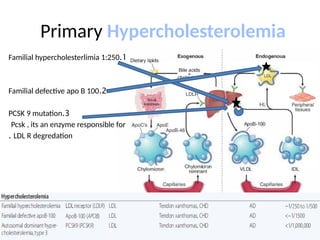
Chylomicron transport fats from the intestinal mucosa to the liver stay
up to 6_10 hours so in fasting state of 12 hour will not detected and
therefore fasting measurement more reliable if fasting 12 hours
.
●
In the liver the chylomicron release triglyceride and some cholesterol
.
●
VLDL carries TG and cholesterol (but contain more TG ) therefore will
elevated markedly especially in hypertriglyceridaemia
●
LDL carries TG and cholesterol (but contain more cholesterol) to the
body's cells therefore markedly elevated in hypercholesterolemia
.
●
When LDL become high , atheroma will form in the vessel and
atherosclerosis will occur
.
●
HDL carry cholesterol to the liver for excretion
●
HDL is able to go and remove cholesterol from the atheroma
●
Atherogenic cholesterol (bad cholesterol) are LDL
●
good cholesterol is HDL
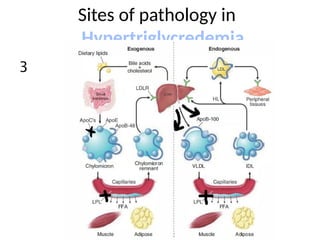
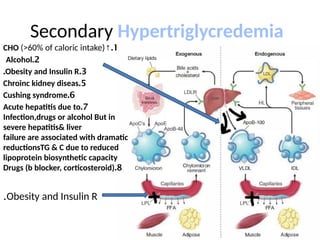
Secondary Hypertriglycredemia
1
.
↑
CHO (>60%of caloric intake)
2
.
Alcohol
3
.
Obesity and Insulin R
.
5
.
Chroinc kidney diseas
6
.
Cushing syndrome
7
.
Acute hepatitis due to
Infection,drugs or alcohol But in
severe hepatitis& liver
failure are associated with dramatic
reductionsTG & C due to reduced
lipoprotein biosynthetic capacity
8
.
Drugs (b blocker, corticosteroid)
Obesity and Insulin R
.
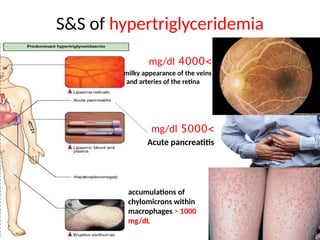
S&S of hypertriglyceridemia
>
4000
mg/dl
milkyappearance of the veins
and arteries of the retina
accumulations of
chylomicrons within
macrophages > 1000
mg/dL
>
5000
mg/dl
Acute pancreatitis
S & Sof hypercholesterolemia
A major risk of CVD,
including myocardial
infarction and stroke , as
well as total mortality
xanthelasma
Corneal arcus
Not significant if in elderly
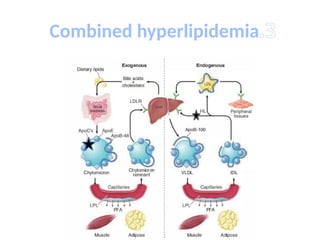
Familial Combined Hyperlipidemia(Fchl)
FCHLis generally characterized by moderate elevations in
plasma levels of triglycerides (VLDL) and cholesterol
(LDL) and reduced plasma levels of HDL-C.
Approximately 20% of patients who develop CHD under
age 60 (premature coronary heart disease) have FCHL
The presence of a mixed dyslipidemia (TG 200 _ 800
mg/dL and total C 200 _400 mg/dL, usually with HDL-C
levels <40 mg/dL in men and <50 mg/dL in women) and
a family history of hyperlipidemia and/or premature
CHD strongly suggests the diagnosis of FCHL
.
Screening and measurement
Plasmalipid and lipoprotein levels should be
measured in all adults , preferably after a 12-h
overnight fast
27.
Evaluation
cholesterol should bemeasured
1
-
Children with parents having hyperlipedemia or
CAD that Developed before 55 years
2
-
any adult with 1st degree relative having lipid
disorder or vascular Disorder
.
3
.
Investigation for every patient with clinical
feature of hyperlipidemia
4
.
Screening for primary and secondary prevention
of cardiovascular disease
.
28.
In most clinicallaboratories, the cholesterol and TGs
in the plasma are measured enzymatically
,
and then the cholesterol in the supernatant is
measured after precipitation of apoB-containing
lipoproteins to determine the HDL-C. The
LDL-C is then estimated using the following equation
:
VLDL C = TG / 5 ( in VLDL TG : C 5 :1 )
LDL-C = total cholesterol - (TG/5) - HDL-C
29.
normal ranges
Total cholesterolless than 200 mg
Mild increase 200 _ 250 mg /dl
Moderate increase 250 _ 300 mg /dl
Severe increase more than 300 mg /dl
LDL C less than 100 mg
HDL C less than 40 mg
Total C/ HDL ratio up to 5 normal
Triglyceride ( fasting ) 35_150 mg/dl
30.
MANAGEMENT OF CHOLESTEROLTO PREVENT
CARDIOVASCU LAR DISEASE
reduce LDL-C substantially reduces the risk of
CVD , including myocardial infarction and
stroke , as well as total mortality
.
It is also worth noting that patients at high risk
for CVD who even have plasma LDL-C levels in
the "normal" or average range also benefit
from intervention to reduce LDL-C levels
31.
1st
Lifestyle
:
1
.
↓
body weight
2
.
↓
saturated fats,trans fats, and cholesterol in
the diet
.
3
.
Regular exercise has relatively little impact on
reducing plasma LDL-C levels , although it
has cardiovascular benefits independent of
LDL lowering
.
32.
Food and additives
4
.
Certainfoods and dietary additives are
associated with modest reductions in plasma
cholesterol levels. Plant stanol and sterol
esters interfere with cholesterol absorption
and reduce plasma LDL-C levels by 10% when
taken three times per day
.
33.
PHARMACOLOGICAL INDICATION FOR
HYPERCHOLESTEROLEMIA
Indication
1
.
patientswith CHD or risk factors even they have
"average" LDL-C levels
.
2
.
To reduce LDL-C to <100 mg/dL in patients with
established CHD
3
.
all patients with markedly elevated plasma levels of
LDL-C levels (>190 mg/dL)
4
.
plasma LDL-C levels between 130 and 190 mg/dL with
The presence of other risk factors such as a low plasma
level of HDL-C (<40 mg/dL)
34.
2nd
line : PharmacologicTherapy to ↓ cholesterol
1
.
HMG-CoA reductase inhibitors (statins)
:
Action
:
①
inhibit HMG-CoA reductase , a key enzyme in cholesterol biosynthesis, lead to ↓
cholesterol s
.
②
statins also increase hepatic LDL receptor activity and accelerated clearance of
circulating LDL
Statin ↓LDL c 60% ↓ TG 40% ↑ HDL 10%
Indication
:
Usually one tablet at night (because there is ↑ action
of Hepatic enzyme at night
)
Simvastatin20-40mg/d maximam 80 mg/d
Most useful and dependent way to
indicate statins uses
depend on guidelines of
British coronary prediction risk chart
If more than 20% risk over next 10 years
35.
Statin SE: dyspepsia,headaches,fatigue,andmuscle
or joint pains. Severe myopathy and even
rhabdomyolysis occur .The risk of myopathy is
increased in
□
older age
,
□
renal Insufficiency
,
□
co_administration of drugs such as erythromycin,
antifungal agents , immunosuppressive drugs
.
*
Interrupt treatment if
1
.
CK is more than 5–10 times the upper limit of normal
(
NR : m 55_170 u/l , f 30 _ 135 u/l
, )
2
.
elevated with muscle symptoms
3
.
ALT is more than 2–3 times the upper limit
36.
2
.
Cholesterole absorption inhibitor: Ezetimibe , blocks
the intestinal absorption of cholesterol by inhibits
NPC1Ll indicated as a combination with statin or
when statin is intolerated . 10 mg lower LDL C 20%
.
3
.
Bile acid sequestrant (resin) : prevent bile acid
absorption thereby reduce liver content of cholesterol
that lead to ↑ LDL receptor and LDL clearance such
cholestyramine,colestipol and colesevelam
SE : bloating and constipation
.
Because bile acidsequestrants are not systemically
absorbed , the cholesterol-lowering drug of choice in
children and in women of childbearing age , who are
lactating or pregnant
.
37.
LDL c APHERESIS
Patientswho remain severely
hypercholesterolemic especially of genetic
cause despite optimally tolerated and
maximam drug therapy are candidates for LDL
apheresis. In this process , the patient plasma
is passed over a column that selectively
removes the LDL and the LDL-depleted plasma
is returned to the patient
.