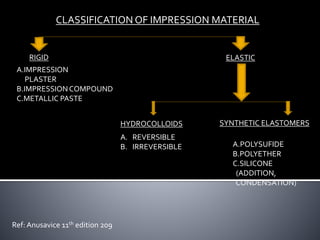
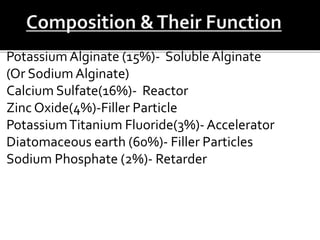
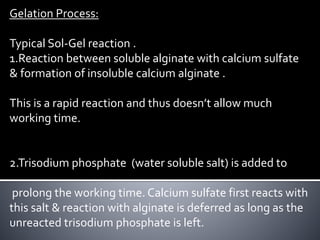
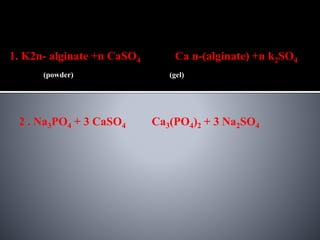
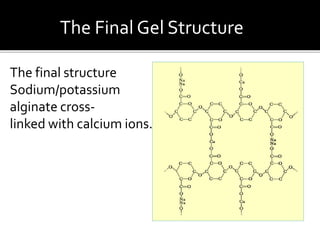
The document discusses the various types of impression materials used in dentistry, focusing on hydrocolloids such as agar and alginate. Key characteristics, classifications, and the gelation process of these materials are detailed, as well as their applications and limitations. It also covers the disinfection processes, dimensional stability issues, and factors affecting the accuracy and effectiveness of dental impressions.












![Physical properties of dental material [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/physicalpropertiesofdentalmaterialautosaved-180818122522-thumbnail.jpg?width=640&height=640&fit=bounds)














![Dental Casting alloys [DENTAL MATERIALS]](https://cdn.slidesharecdn.com/ss_thumbnails/castingalloysbp-200331155134-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




