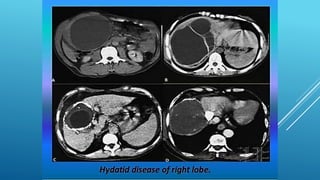
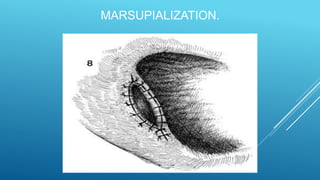
This document discusses the surgical management of hydatid cysts of the liver. It notes that surgery is the treatment of choice for uncomplicated cysts and aims to inactivate cyst contents, prevent spillage, eliminate cyst elements, and manage residual cavities. Surgical techniques discussed include excision, marsupialization, drainage, omentoplasty, and partial hepatectomy. Laparoscopic removal using specialized instruments is also described. Percutaneous aspiration, injection with scolicidal agents, and reaspiration (PAIR) is discussed as an alternative to surgery for selected cases.





















































![Urinary Diversion after cystectomy [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urinarydiversionedmond-140716212817-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















































