LEARNING OBJECTIVES
• Atthe end of the session students should be able to:
1. Identify the bone with side determination of humerus
2. Describe different bony landmarks of it
3. Explain different muscles attachment
4. Describe different clinical aspects of bone injuries
4.
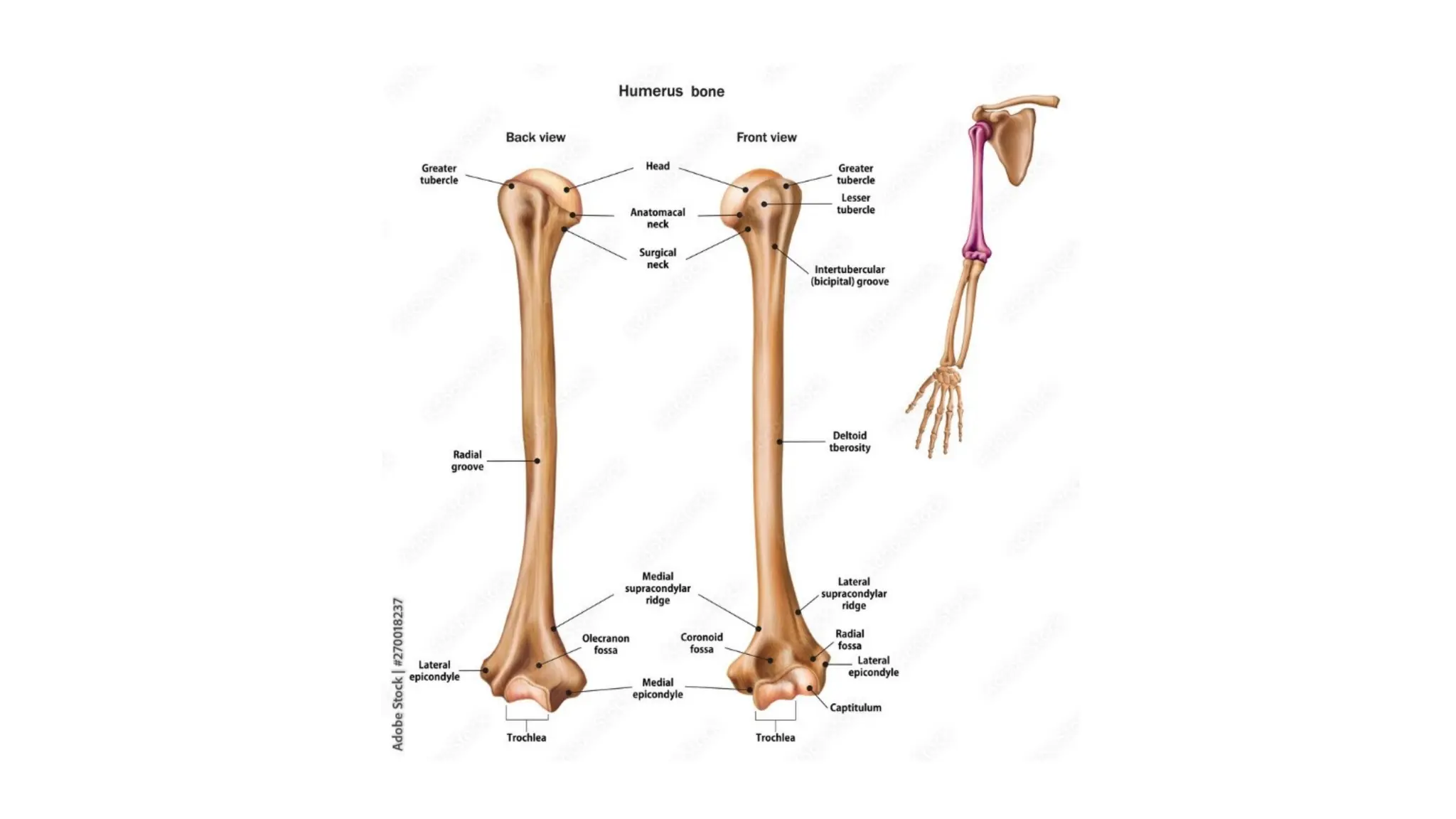
HUMERUS
• Bone ofthe Arm or Brachium
• Long bone
• Has two ends and a shaft
• Above forms Shoulder joint (Glenohumeral joint)
• Below forms Elbow joint
5.
SIDE DETERMINATION
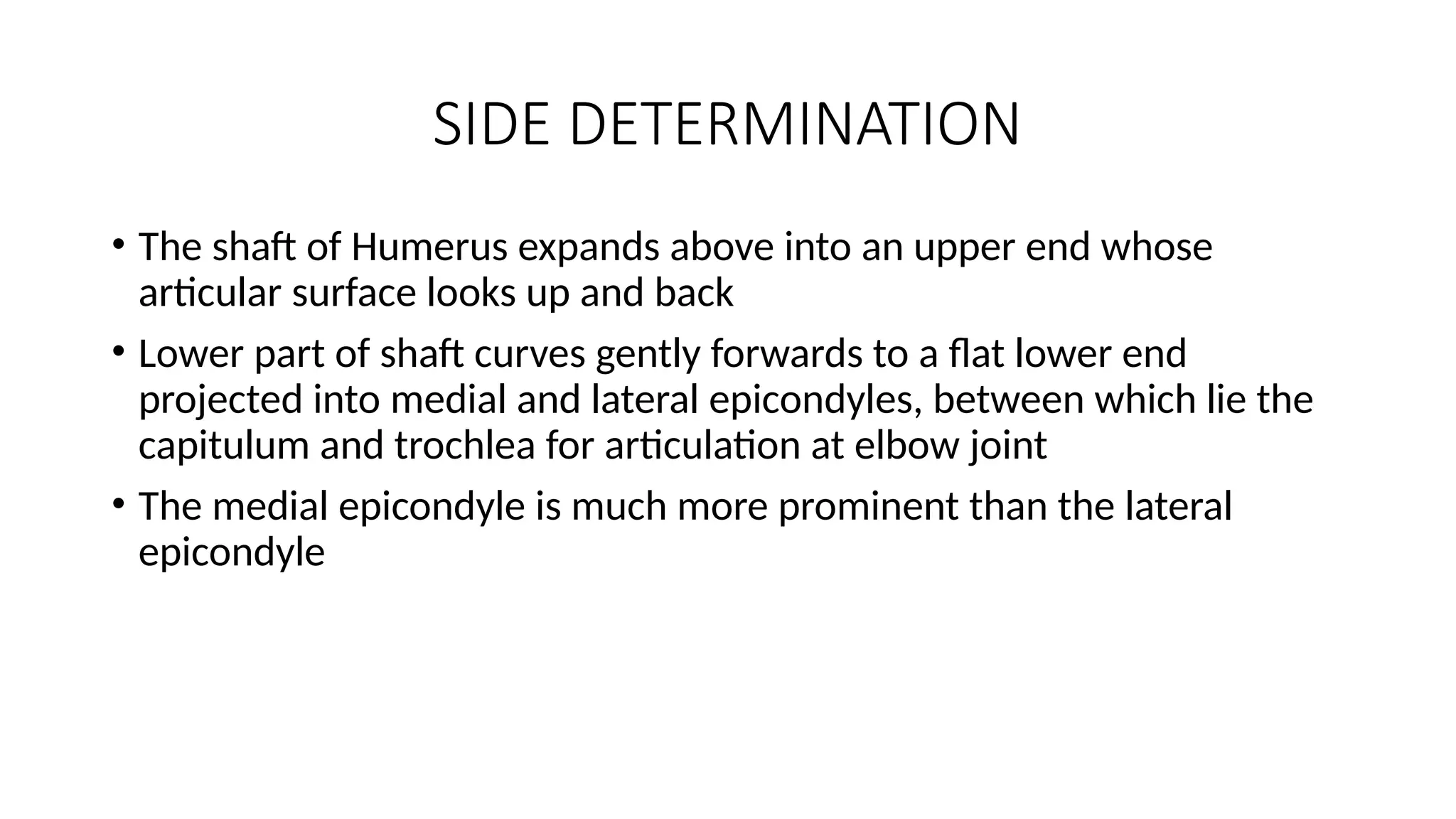
• Theshaft of Humerus expands above into an upper end whose
articular surface looks up and back
• Lower part of shaft curves gently forwards to a flat lower end
projected into medial and lateral epicondyles, between which lie the
capitulum and trochlea for articulation at elbow joint
• The medial epicondyle is much more prominent than the lateral
epicondyle
7.
UPPER END
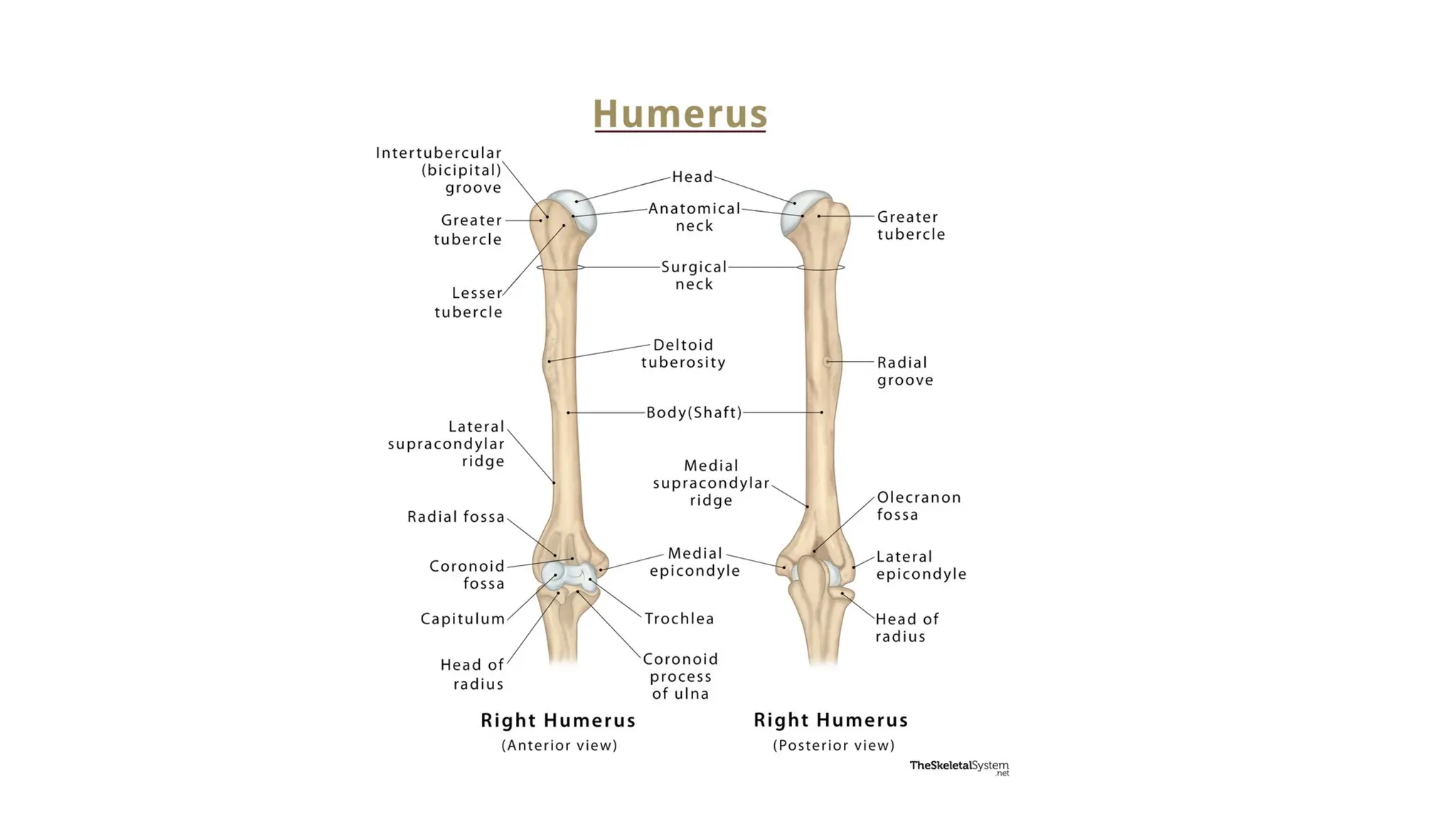
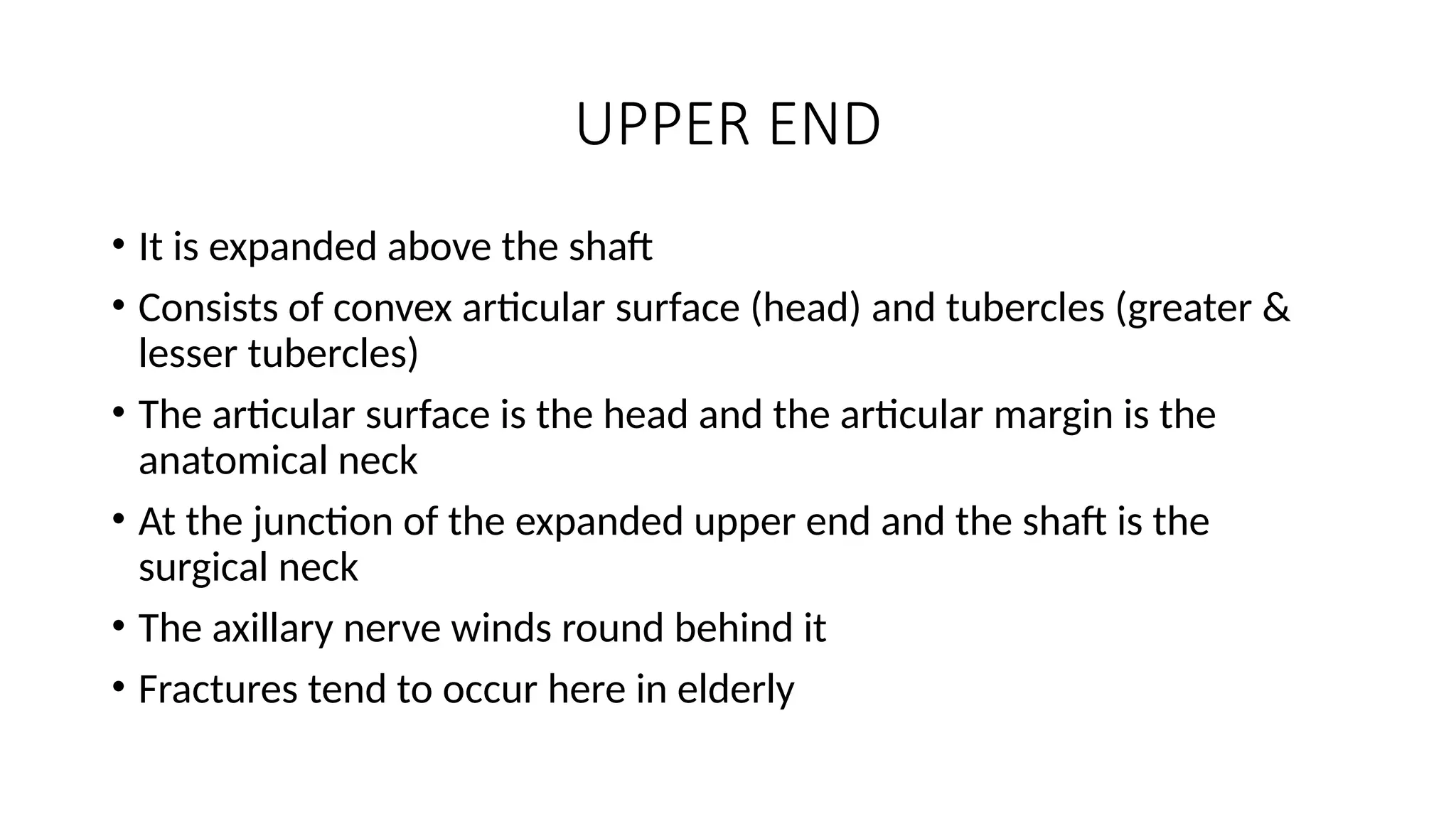
• Itis expanded above the shaft
• Consists of convex articular surface (head) and tubercles (greater &
lesser tubercles)
• The articular surface is the head and the articular margin is the
anatomical neck
• At the junction of the expanded upper end and the shaft is the
surgical neck
• The axillary nerve winds round behind it
• Fractures tend to occur here in elderly
9.
HEAD
• The articularsurface forms about one-third of a sphere and is about
four times the area of glenoid cavity of scapula
• It is coated with hyaline cartilage
10.
LESSER TUBERCLE
• Alsocalled Tuberosity
• Projects prominently forwards
• Continued downwards as medial lip of bicipital sulcus or groove
• Tendon of subscapularis is inserted on it
• Teres major on medial lip
11.
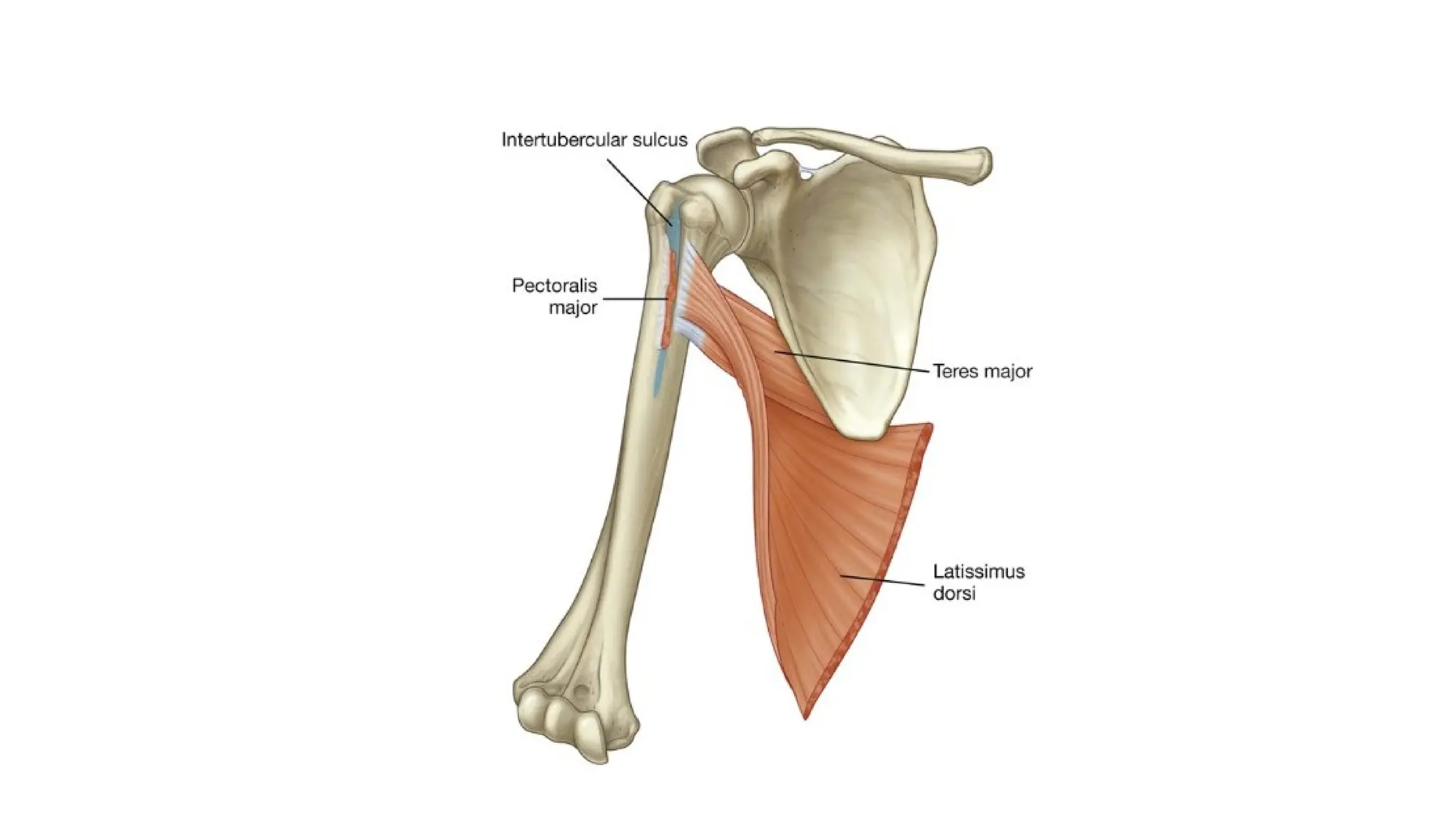
BICIPITAL GROOVE /SULCUS
• Also called intertubercular sulcus
• It lies on the anterior surface of upper end
• It is bridged above by transverse humeral ligament
• Deep to it long tendon of biceps leaves the joint
• The floor of sulcus receives the tendon of latissimus dorsi muscle
• Medial lip has teres major
• Lateral lip has pectoralis major
• Lady between two majors
14.
GREATER TUBERCLE
• Alsocalled Tuberosity
• It is bare except at its projecting junction with head
• Where there are three smooth facets for insertion of tendons of scapular
muscles:
1. Superiorly: Supraspinatus
2. Behind: Infraspinatus
3. Posteriorly: Teres minor (below this tendon the bone lies in contact with
axillary nerve and its vessels)
• The lateral lip of bicipital sulcus extends down from the anterior margin of
greater tubercle and receives the tendon of pectoralis major
15.
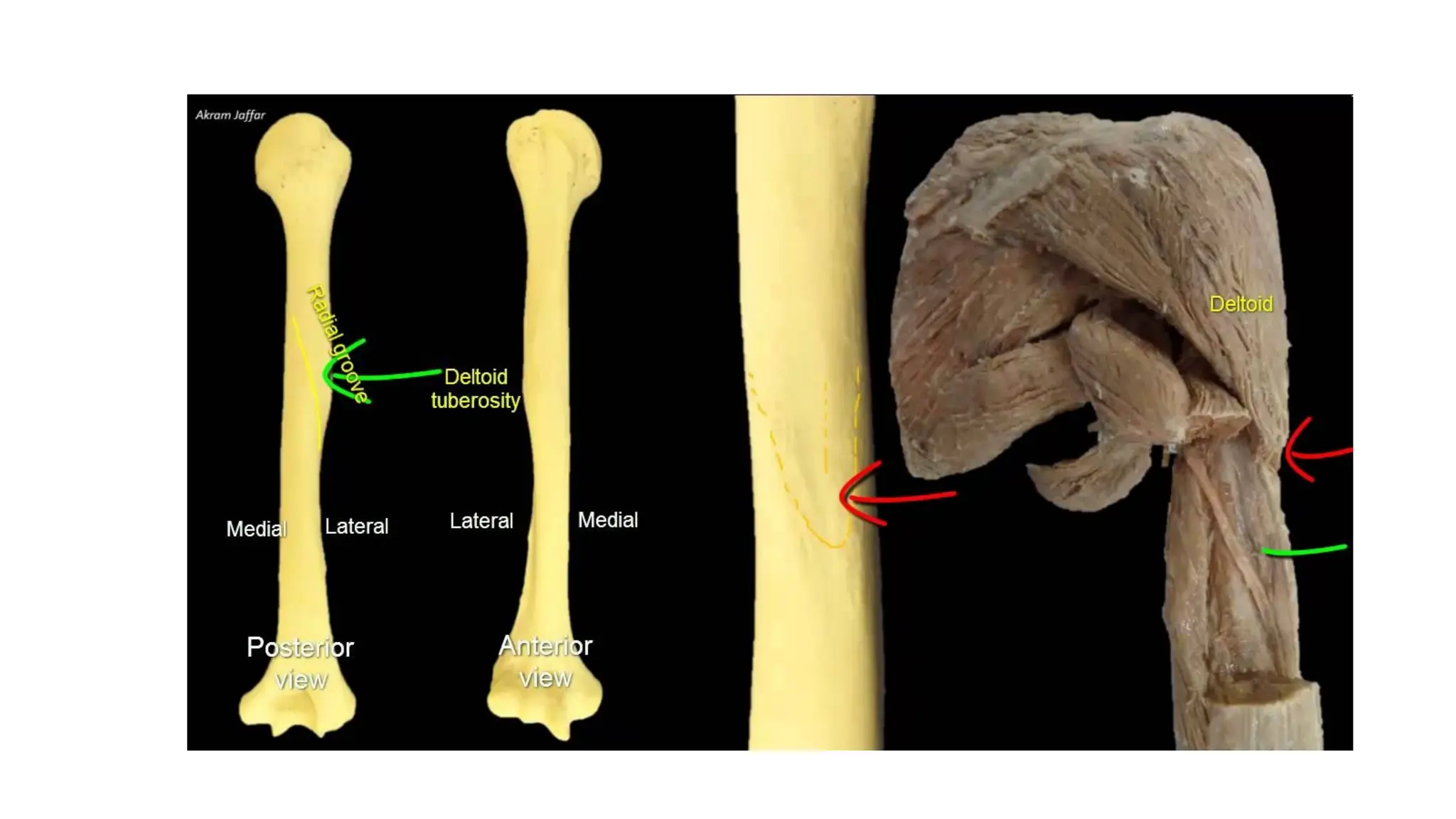
SHAFT
• Much ofthe shaft is triangular in section
• The deltoid tuberosity is at the middle of lateral side of shaft
• It is a V-shaped prominent ridge
• Below the deltoid tuberosity the lower end of radial groove spirals down
• The lower margin of groove continues as the lateral supracondylar ridge,
which runs down to lateral epicondyle
• The less marked medial supracondylar ridge runs down to the prominent
medial epicondyle
• Radial nerve and profunda brachii vessels lie in radial groove
17.
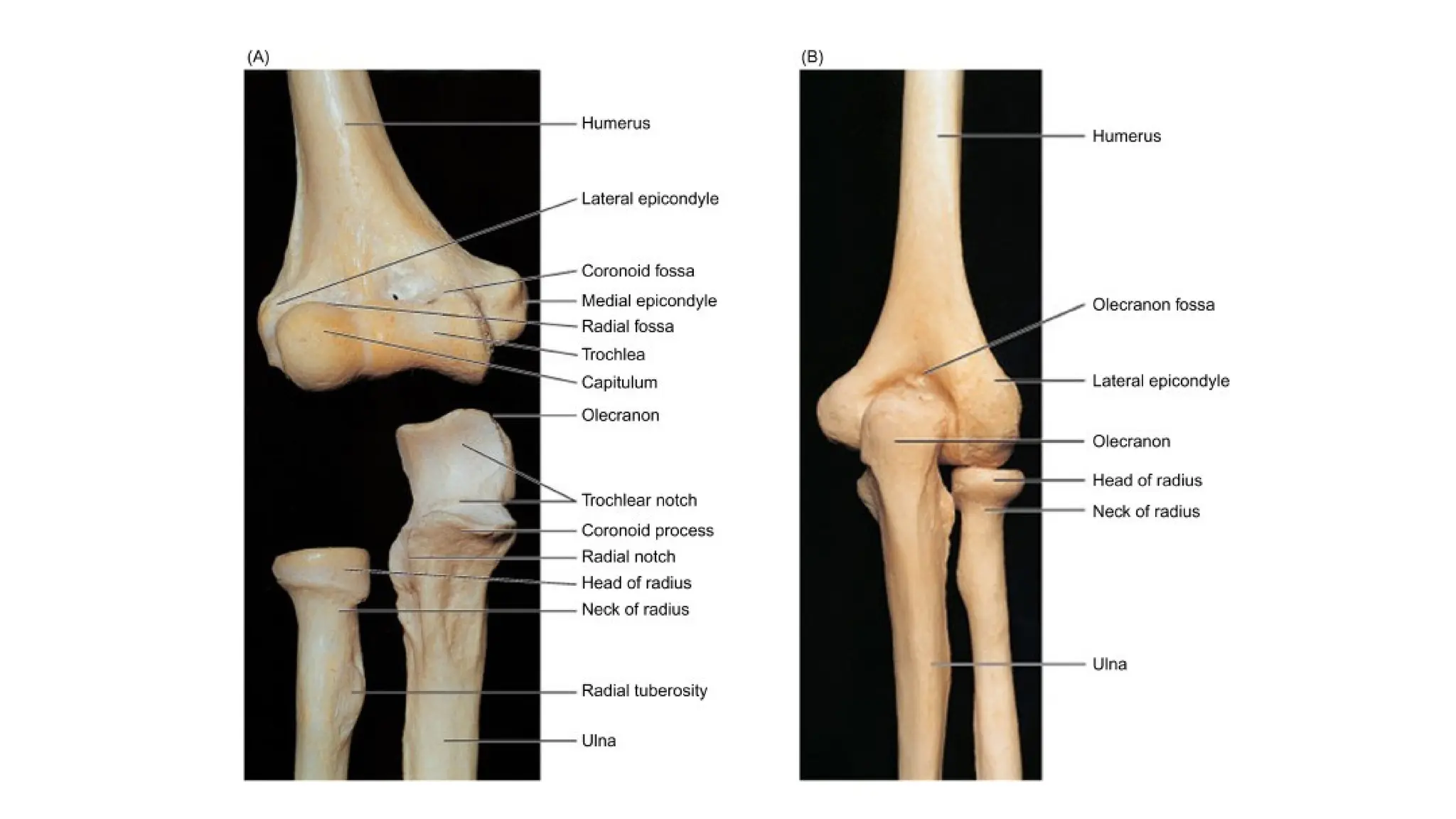
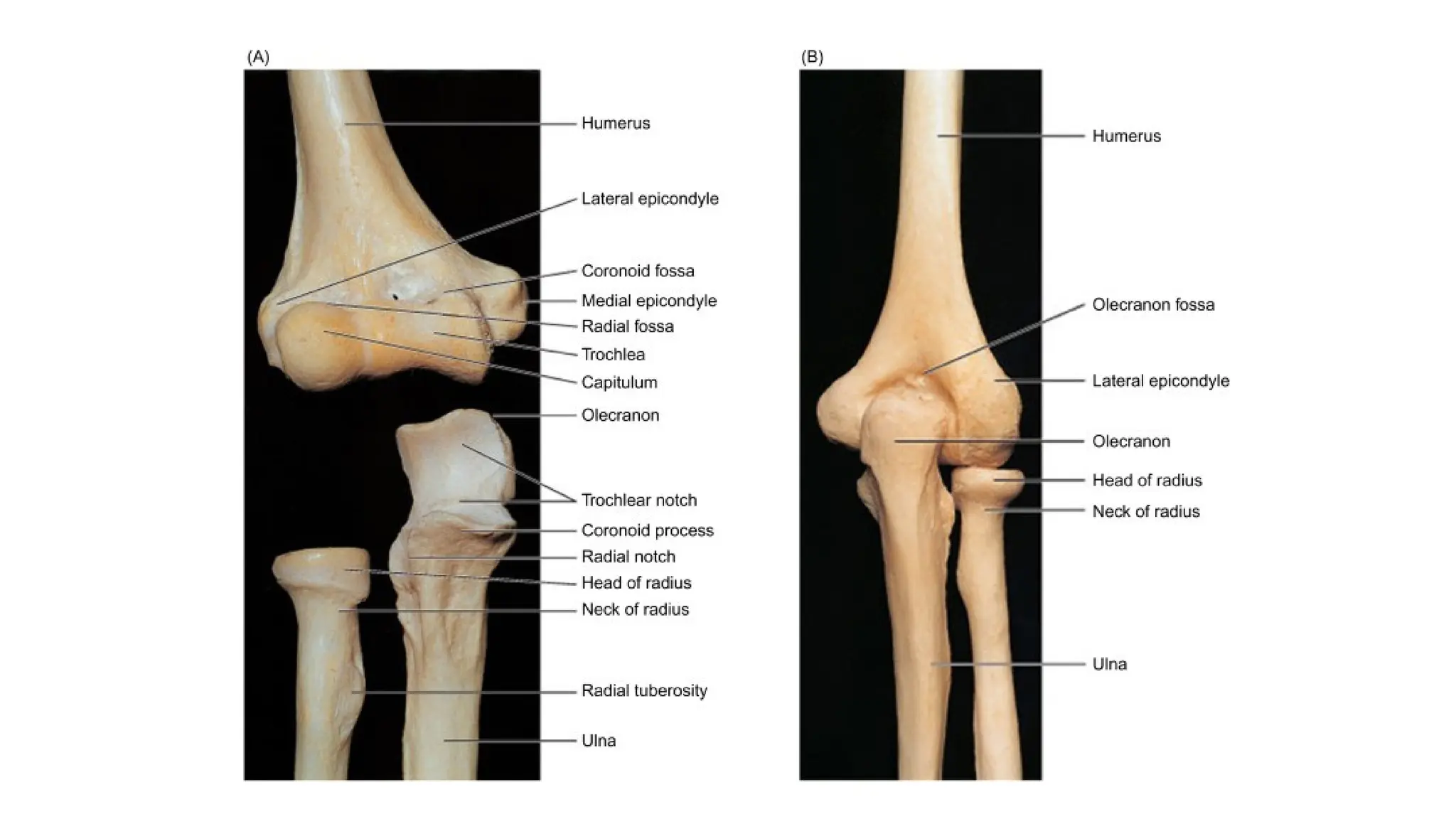
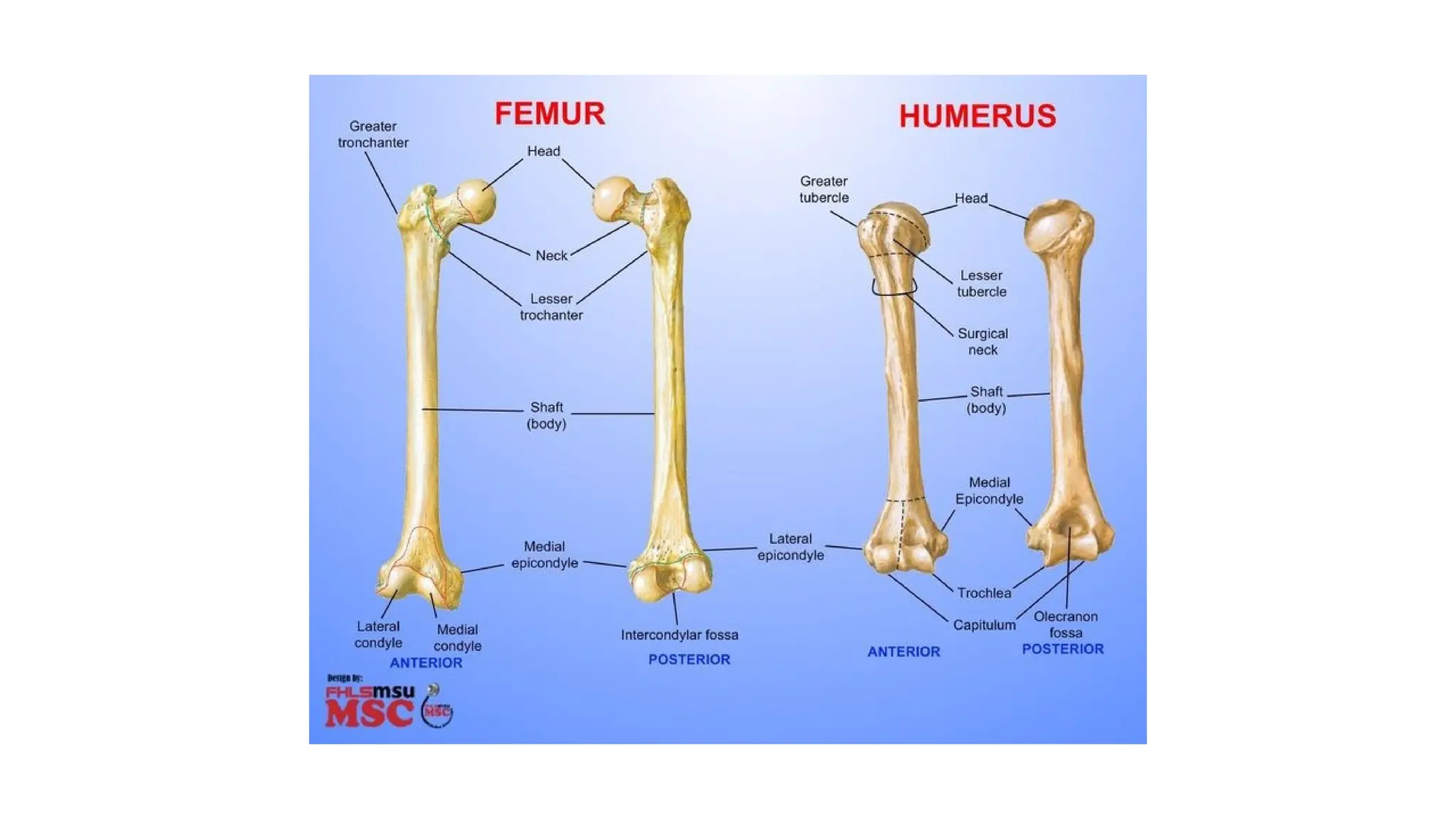
LOWER END
• Thisend of Humerus carries the articular surface for elbow joint
• It is projected into medial and lateral epicondyles for attachment of muscles
for the flexor and extensor compartments of the forearm
• The articular surface shows the conjoined capitulum and trochlea
• Capitulum for articulation with head of radius
• Trochlea, unlike capitulum, extends also to posterior surface
• Its medial margin is a sharp ridge curving prominently from front to back
around lower end of Humerus
• The medial part of trochlea is at a more distal level than capitulum, which is
a causative factor for the carrying angle at elbow
19.
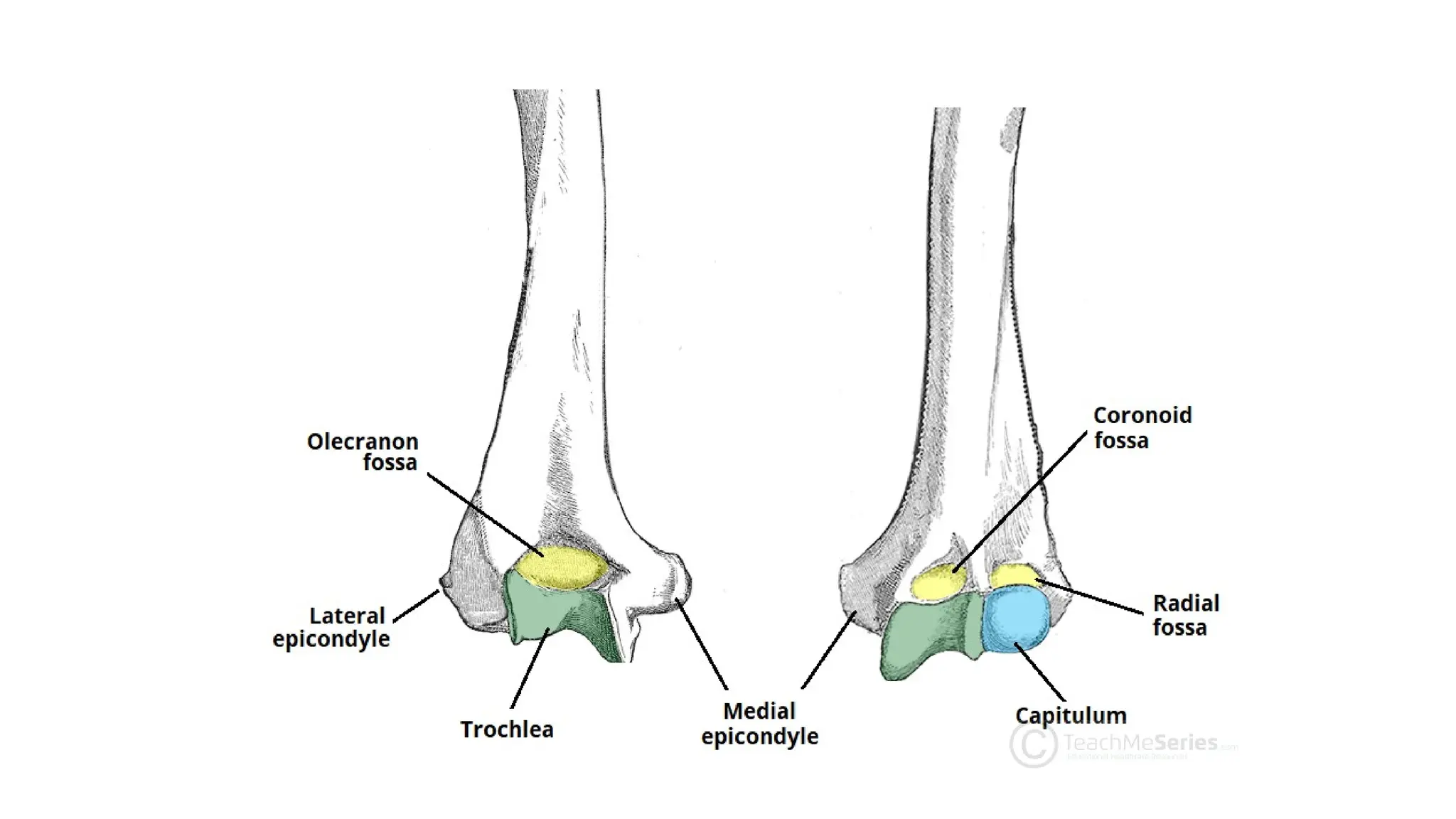
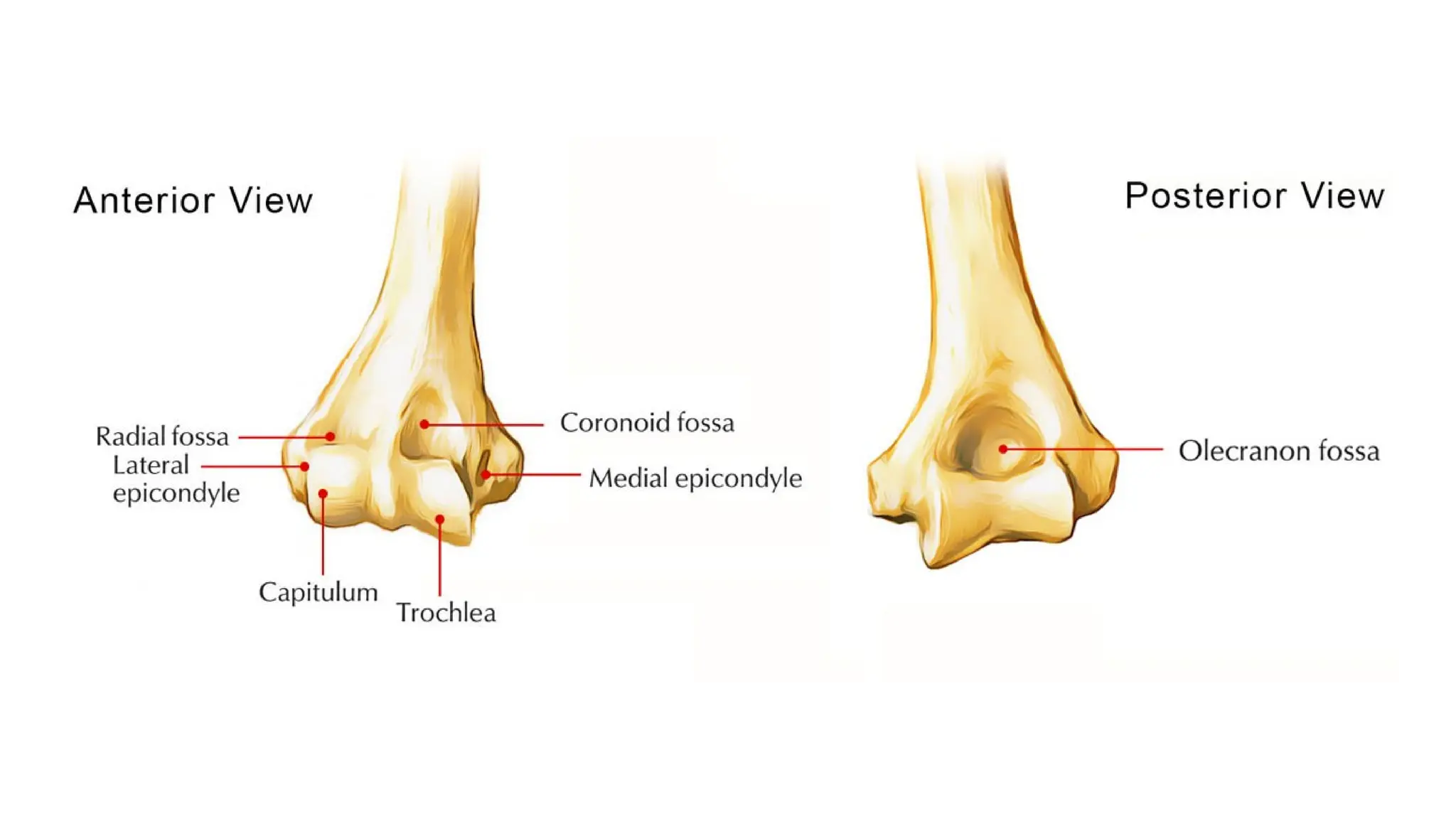
LOWER END
• Theanterior surface of shaft of lower end of Humerus shows a
shallow coronoid fossa above the trochlea and a shallow radial fossa
above the capitulum
• A deep olecranon fossa is seen on the posterior surface
21.
MEDIAL EPICONDYLE
• Hasa smooth facet on its anterior surface for common flexor origin of
forearm muscles
• Pronator teres arises from medial supracondylar ridge just above this
• Posteriorly between the epicondyle and curving ridge of trochlea is a
groove which lodges ulnar nerve
23.
LATERAL EPICONDYLE
• Ithas a smooth facet on its anterior surface for common extensor
origin of forearm muscles
• Above this is lateral supracondylar ridge from which arises
brachioradialis from upper two thirds and extensor carpi radialis from
lower one third
• Anconeus arises from posterior surface
25.
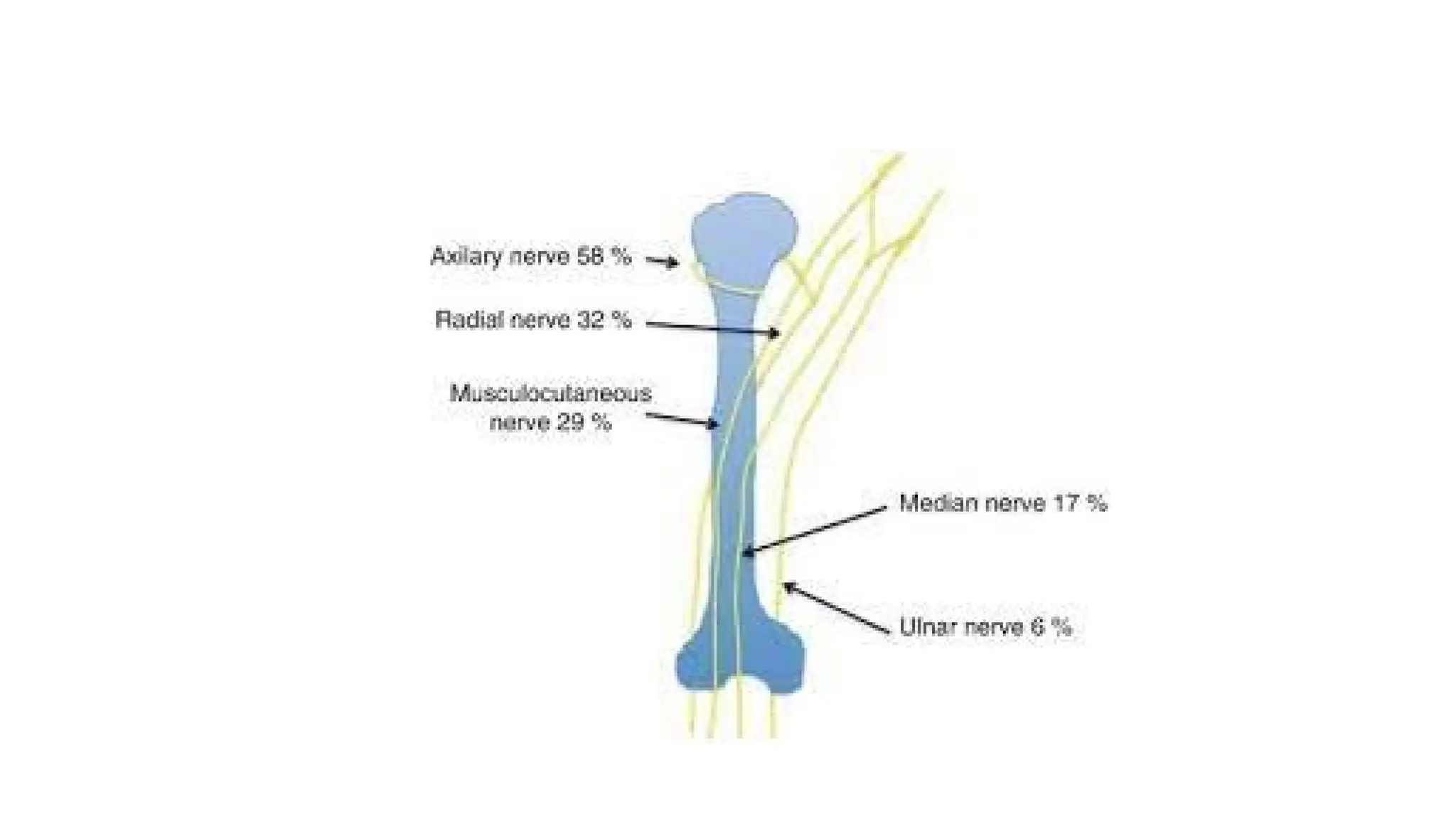
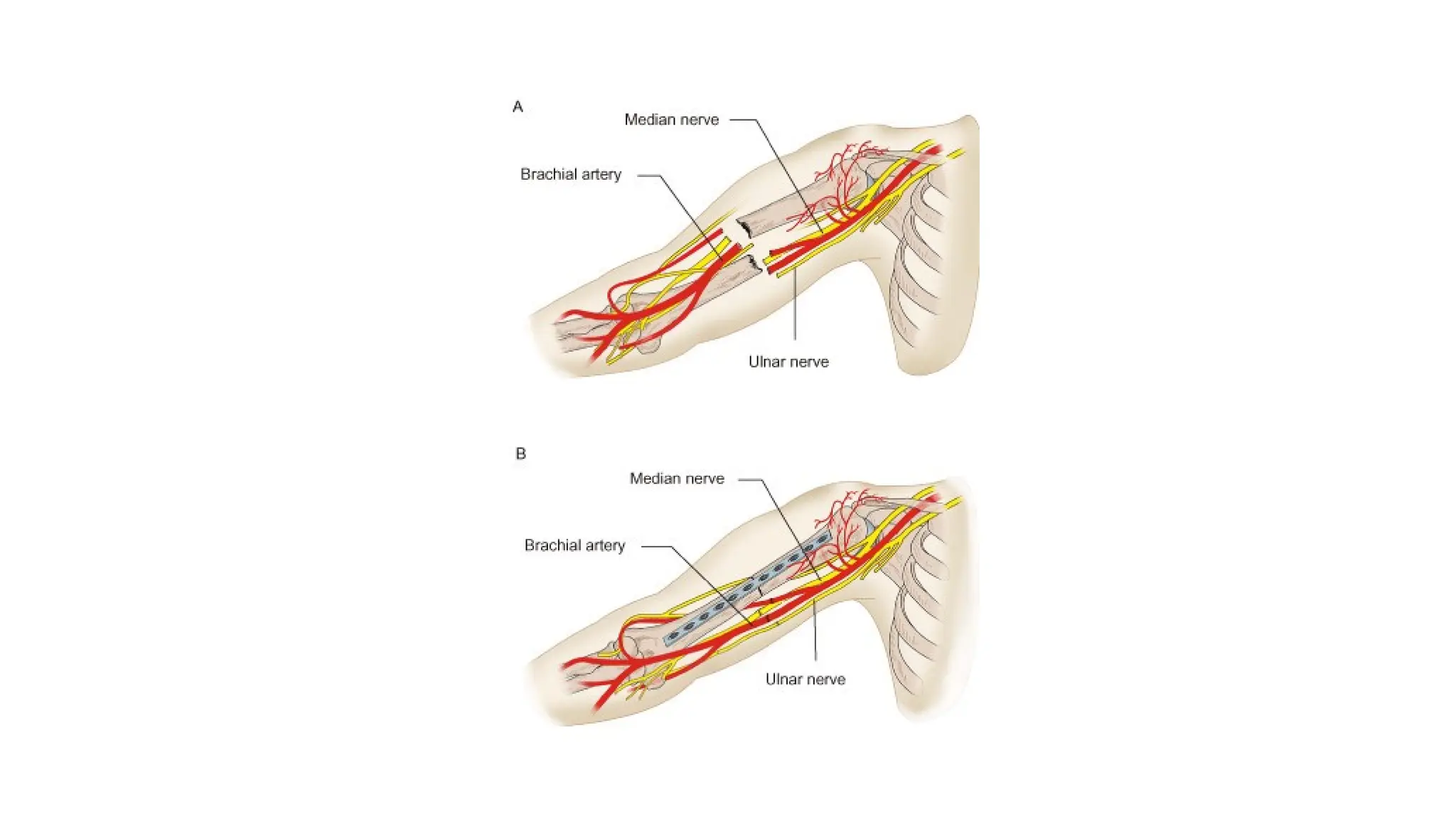
APPLIED
• The shaftcan be exposed from the front by opening up the
deltopectoral groove
• The incision is made anterolaterally and obliquely towards middle of
front of shaft to preserve brachial artery and median nerve
• The radial nerve must be in mind at lateral side of lower part of shaft
28.
OSSIFICATION
• A primarycentre appears in the centre of shaft at eighth week of
intrauterine life
• Upper and lower ends are cartilaginous at birth
• Three secondary centres appear at upper end for head, greater, and
lesser tubercles in first few years after birth
• They fuse into a single bony epiphysis
• This is growing end of bone and fusion occurs with shaft at about 20
years
29.
OSSIFICATION
• Four secondarycentres appear at lower end
• Three form trochlea, capitulum, and lateral epicondyle
• Fuse into a single epiphysis, which fuses with the shaft at about 15
years
• Medial epicondyle remains as a separate center, which fuses with a
downward projection of shaft at about 20 years
• This late fusion needs to be kept in mind when interpreting
radiographs of elbow region in adolescents