Downloaded 11 times
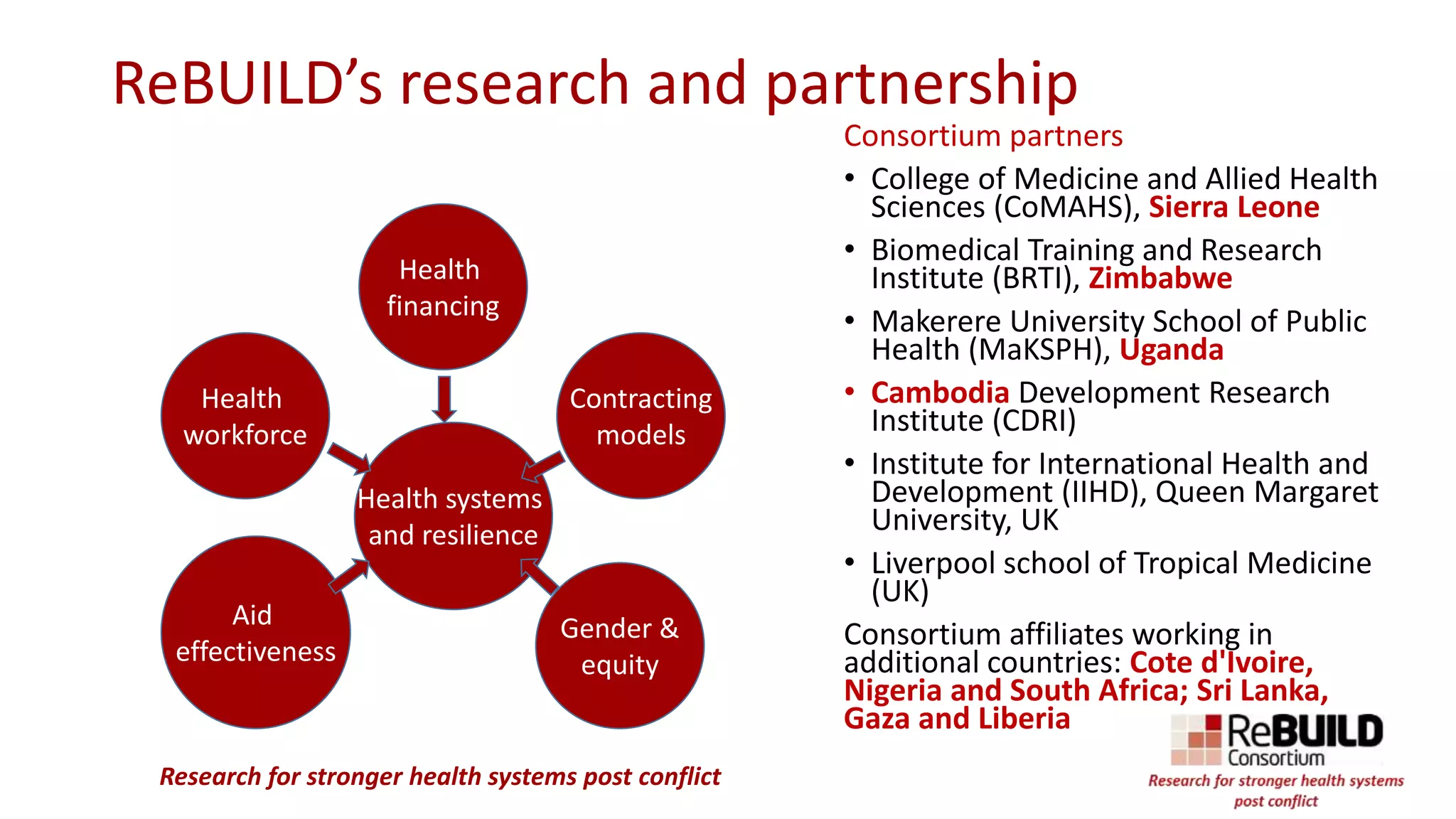
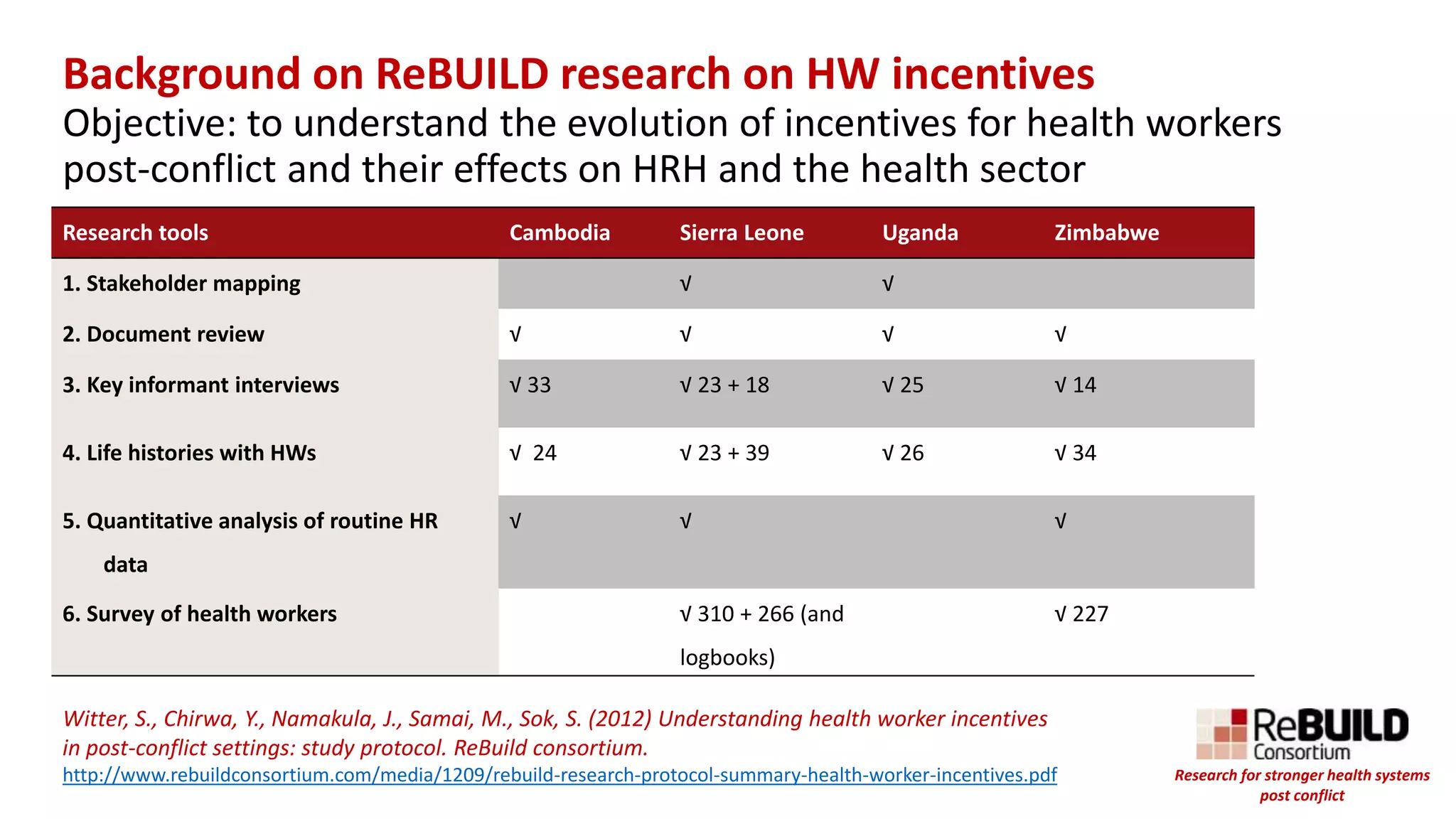
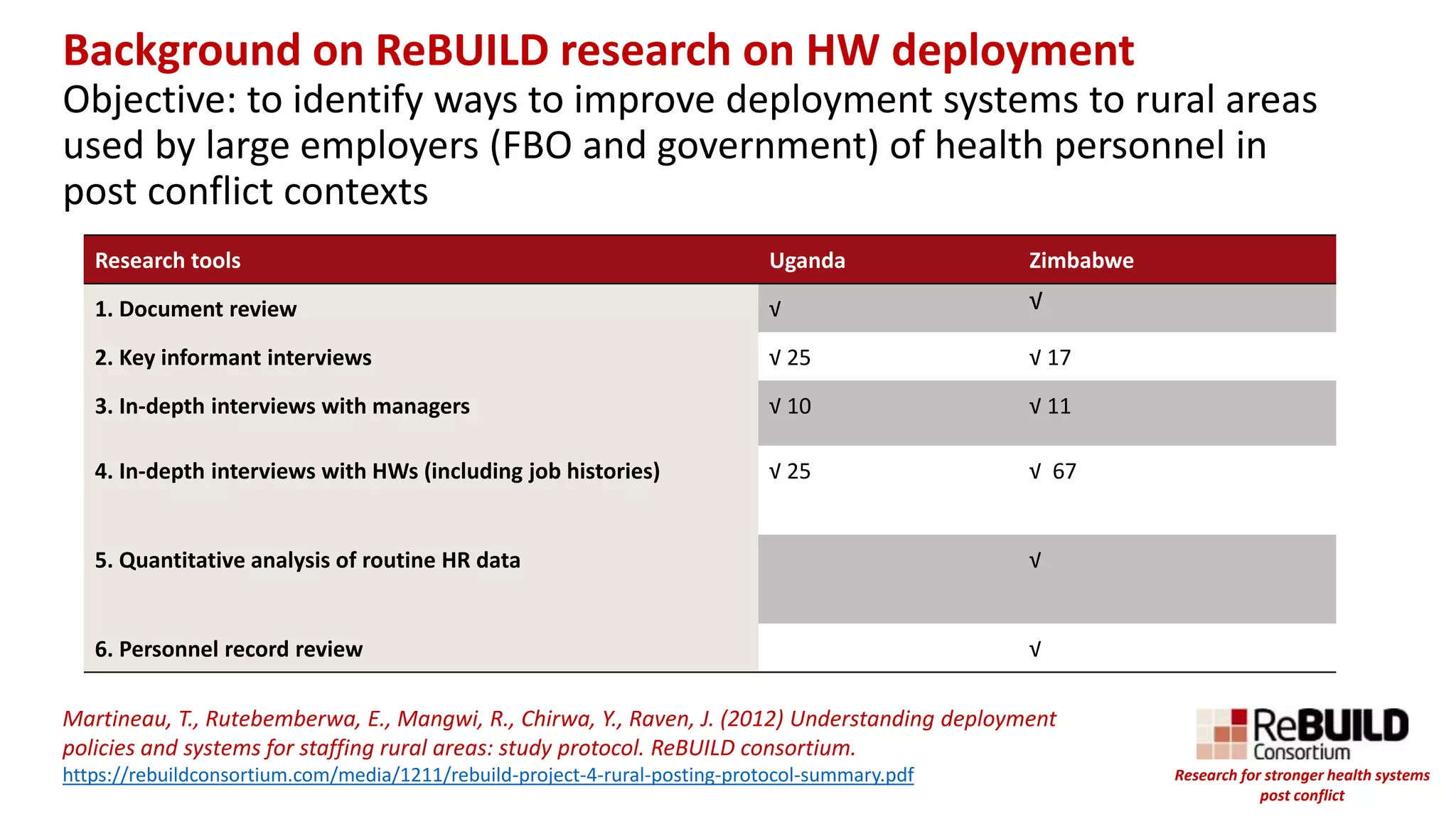


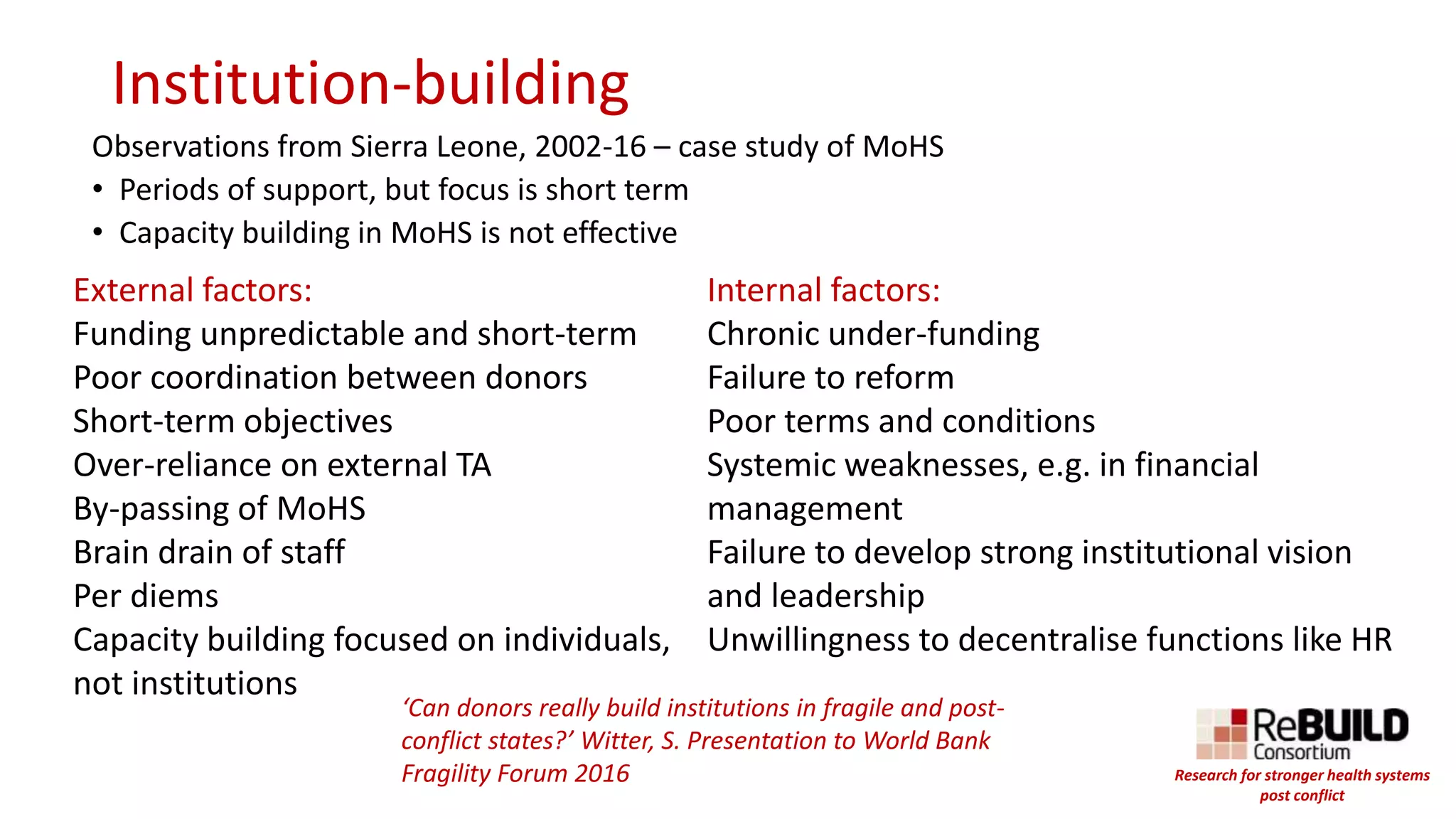

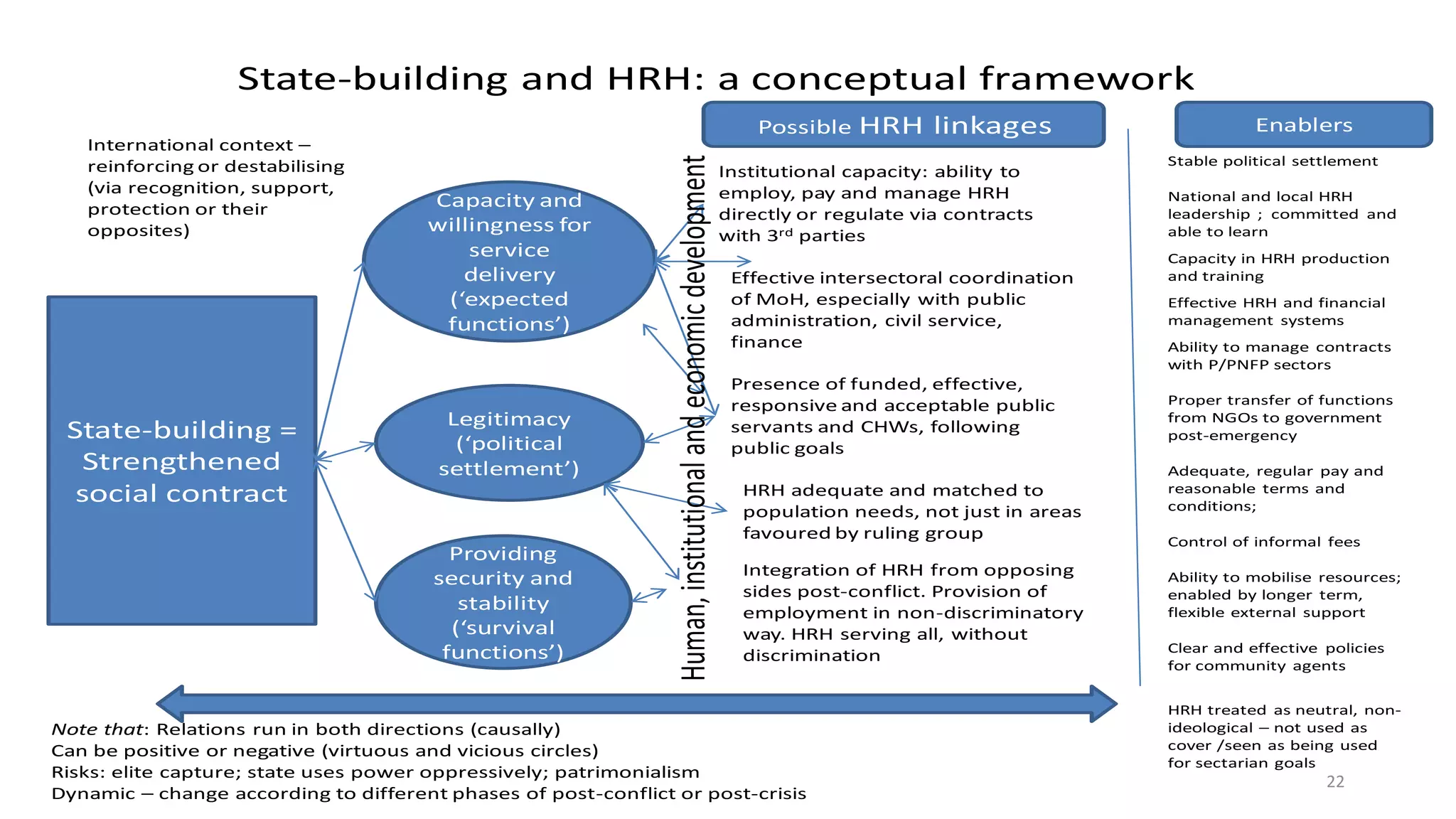




The document presents findings from research on health worker dynamics in post-conflict contexts, focusing on issues of recruitment, retention, and the impact of gender on health workforce policy. It emphasizes the importance of understanding health worker incentives and the innovative strategies used by staff to cope with crises. The research highlights the complexities of health system reform in fragile environments, stressing the need for long-term planning and institutional capacity building to sustain health services.