How to Teach Using Simulation in Healthcare 1st Edition Mike Davis
How to Teach Using Simulation in Healthcare 1st Edition Mike Davis
How to Teach Using Simulation in Healthcare 1st Edition Mike Davis
How to Teach Using Simulation in Healthcare 1st Edition Mike Davis
How to Teach Using Simulation in Healthcare 1st Edition Mike Davis
1.
Read Anytime AnywhereEasy Ebook Downloads at ebookmeta.com
How to Teach Using Simulation in Healthcare 1st
Edition Mike Davis
https://ebookmeta.com/product/how-to-teach-using-simulation-
in-healthcare-1st-edition-mike-davis/
OR CLICK HERE
DOWLOAD EBOOK
Visit and Get More Ebook Downloads Instantly at https://ebookmeta.com
How to Teach
UsingSimulation
in Healthcare
Mike Davis
Freelance consultant in continuing medical education, UK
Jacky Hanson
Lancashire Teaching Hospitals, UK
Mike Dickinson
Blackpool Teaching Hospitals, UK
Lorna Lees
Lancashire Teaching Hospitals, UK
Mark Pimblett
Lancashire Teaching Hospitals, UK
v
Contents
List of figures,vii
List of tables, ix
About the authors, xi
Preface, xv
Chapter 1: Introduction, 1
Chapter 2:
Simulation‐based medical education (SBME):
some specifics, 3
Chapter 3:
Simulation in (medical) education: some
background, 13
Chapter 4: Equipment in SBME: more than just a mannikin?, 27
Chapter 5: Physical and psychological realism, 37
Chapter 6: Simulation mapping and scenario design, 45
Chapter 7: Running a simulation session: some practicalities, 55
Chapter 8: Formative assessment and feedback, 65
Chapter 9: Summative assessment, 73
Chapter 10:
Human factors, ergonomics and non‐technical
skills, 83
Chapter 11: Five case examples, 97
Chapter 12: Using new technology to enhance learning, 119
Chapter 13: Commissioning a simulation centre, 139
9.
vi Contents
Chapter 14:Training for simulation faculty, 151
Chapter 15: Conclusions and next steps, 157
Chapter 16: Annotated bibliography, 159
Index, 163
10.
vii
List of figures
3.1Experiential learning cycle, 14
3.2 Zone of proximal development (ZPD), 19
3.3 Activity theory, 23
3.4 Activity theory within emergency medicine, 24
3.5 Activity theory within simulation suite, 24
4.1 Part task trainer for cannulation, 30
6.1 Achieving conscious competence, 46
6.2 Generic competencies for specific scenarios, 47
6.3 Specific competencies related to management of
shocked patient, 48
6.4 Example scenario, 49
7.1 The SaIL Diamond, 60
7.2 Sample evaluation form, 62
8.1 ALS treatment of a shockable rhythm, 66
9.1 Miller’s pyramid, 74
9.2 Component elements of medical expertise, 75
10.1 Reported degree of harm to patients NPSA 2011–12 data, 84
10.2 Reported incidence types in England NPSA
July 2011–June 2012, 84
10.3 SEIPS, 86
10.4 Model of communication, 91
11.1 The zone of simulation, 99
11.2 The Preston zone of simulation, 100
11.3 Initial steps in planning to receive a trauma patient, 111
11.4 The team approach to the primary survey, 112
11.5 Individual patient pathway, 113
12.1 Dynamic and static elements of the Asthma scenario, 125
12.2 iCoda template for asthma, 125
12.3 A tagged timeline, 126
12.4 Marking matrix, 126
12.5 iCoda template for non-technical skills, 128
11.
viii List offigures
13.1 Part task trainer, 142
13.2 Multipurpose space, 143
13.3 Adaptation of existing facility, 144
13.4 Plans for customised simulation centre, 145
13.5 Wet room, 146
12.
ix
List of tables
8.1Distinction between feedback and debrief, 67
10.1 Styles and definitions in leadership, 93
10.2 Situational leadership, 94
11.1 Structure of undergraduate simulation experience, 98
11.2 Sample issues identified for debrief, 107
11.3 Number of actions against learning outcomes of the patient safety
programme, 107
11.4 Examples of good practice, 108
11.5 Number of areas of good practice against learning outcomes of the
patient safety programme, 108
12.1 Use of social media, 132
14.
xi
About the authors
MikeDavis PhD MEd DASE Cert Ed FAcadMEd is a freelance consultant in
continuing medical education, working mainly within the life support
community and with extensive experience in the UK and throughout the
world. He is the author of two other books in the How to … series and other
education texts. He has written and refereed for a variety of medical educa-
tion journals and is on the Editorial Board of BMJ‐STEL. He has been lead
educator for the Advanced Life Support Group since 1995 and for six years,
he was educational adviser to the PHROST project based at Lancashire
Teaching Hospitals NHS Trust. He is also an educator with ATLS, IMPACT
and ETC. He is a Fellow of the Academy of Medical Educators and an
Honorary Senior Lecturer in Medical Education at Keele University.
Jacky Hanson BSc MBChB FRCS FRCEM is an emergency medicine
consultant, Director of Simulation and Associate Undergraduate Dean at
Lancashire Teaching Hospitals. She has interests in educational research,
human factors and ergonomics including non‐technical skills and develop-
ing simulation training regionally and nationally. She has presented on simu-
lation to national and international audiences. She was Director of CPD and
Revalidation for RCEM and is an examiner for FRCEM and a member of the
RCEM simulation group. Jacky contributed to the design and development
of the simulation centre at Lancashire Teaching Hospitals NHS Trust and has
been clinical lead since its inception.
MikeDickinsonRGNDipIMC(RCSEdinburgh)IFNAPGDipFETCiscurrently
Manager of the Simulation and Clinical Skills unit at Blackpool Teaching
Hospitals NHS Foundation Trust. He qualified as an RGN in 1982 and has
worked in various areas of the UK and internationally, including the USA
and Africa. He has extensive knowledge of training design and programme
development in the critical care field. Mike is an examiner for the Faculty of
Pre‐Hospital Care (Royal College of Surgeons Edinburgh) and is an instruc-
tor in multiple internationally recognised life support courses. He has
presented internationally on various aspects of SBME.
15.
xii About theauthors
Lorna Lees SRN qualified as a registered nurse in 1982 and eventually
became ward sister on a neurology ward before leaving nursing to bring up
her family. Her involvement with SBME started in 2011 when she was
appointed to the role of simulation technician and subsequently training
administrator and co‐ordinator. She continues to play an active role in the
provision of SBME not only as a training co‐ordinator but also assisting with
facilitation.
Mark Pimblett RODP contributed to the design and development of the
state‐of‐the‐art Lancashire Simulation Centre (based at Lancashire Teaching
Hospitals) where he currently works as a high‐tech clinical skills facilitator.
His professional background is in operating department practice, specialis-
ing mainly in anaesthesia and emergency medicine. He crossed over into
medical education in 2003, incorporating his clinical experience and his
interest in technologies to establish human patient simulation training within
the north west region of England. Mark is an international speaker on all
aspects of human patient simulation, including simulation centre design,
scenario development, performance analysis and technology innovation. He
is an expert trainer in human factors and a specialist in video debrief and
feedback.
We would also like to thank the following:
Chris Busuttil FRCSEd (AE) FRCEM qualified in 1996 at Imperial College
School of Medicine, London. He was first appointed as a consultant in 2008
and currently works in emergency medicine at the Queen Alexandra
Hospital, Portsmouth. He is an examiner and Simulation NTS Committee
member (Wessex Region), Royal College of Emergency Medicine. Chris
wrote the section in Chapter 12 on ‘Ethical considerations in the video
recording of simulation’.
Alison Gale MB ChB FRCOG MMedEd FAcadMEd is a consultant obste-
trician and gynaecologist and the Director of Postgraduate Medical
Education at Lancashire Teaching Hospitals. She has educational leadership
responsibilities at local, regional and national levels, including Simulation
Lead for the Royal College of Obstetricians and Gynaecologists (2009–2016)
and NACT UK Council representative for the North West (2014–2016). She
is a current MRCOG Examiner and a member of the MRCOG Part 3
subcommittee.
Jo‐Anne Halliwell RGN MSc BSc DPSN PG Cert is currently working as
clinical improvement lead for adult and long‐term conditions as part of the
community nursing team and has extensive experience of working in various
16.
About the authorsxiii
areas of the NHS, including operating departments and anaesthetics. As a
practice development nurse and lead facilitator in simulation‐based medical
education, she helped commission the simulation unit at Blackpool Teaching
Hospital NHS Foundation Trust. She has extensive experience of programme
design and risk management assessment and, with Simon Tucker, she wrote
‘Enhancing patient safety through multidisciplinary in situ simulation’ in
Chapter 11.
Helen Higham MBChB FRCA SFHEA has been a consultant anaesthetist at
the Oxford University Hospitals NHS Foundation Trust since 2001 and is a
senior clinical research fellow in the Nuffield Department of Clinical
Neurosciences at the University of Oxford. She is Director of the University
of Oxford’s Simulation Centre (www.oxstar.ox.ac.uk/) and is co‐director of
the Patient Safety Academy, providing training and support to healthcare
professionals in the application of human factors to improve quality and
safety across the Thames Valley LETB (www.patientsafetyacademy.co.uk/).
She is a current executive member and immediate past president of the
Association for Simulated Practice in Healthcare (ASPiH) in the UK.
Alison Quinn MB ChB FRCA is an ST7 in Anaesthetics in the North West
Deanery. She has previously completed a fellowship in Medical Education
and Simulation with LTHTR and the University of Manchester. She now
holds an honorary lecturer post with the assessment team at Manchester
Medical School where she is currently lead for the year 4 ‘Movement’ OSCE.
Alison holds a Postgraduate Diploma in Clinical Education and her main
areas of interest include assessment and human patient simulation. She wrote
Chapter 8 on formative assessment.
Libby Thomas BMBS MCEM PGDipClinEd is an emergency medicine spe-
cialist trainee and PhD student in medical education focusing on interprofes-
sional full patient simulation for undergraduates. She is module lead for
Simulation in Clinical Education at King’s College London. Libby made useful
suggestions and introduced us to the idea of sociological realism (Chapter 5).
Simon Tucker BSc MBChB MRCS (Edinburgh) FCEM is a consultant in
emergency medicine at Blackpool Teaching Hospitals. He is an ALS and
APLS instructor and through these had some experience of low‐fidelity
simulation. His introduction to high‐fidelity simulation occurred when he
volunteered to assist in the undergraduate and Foundation SBME pro-
gramme. He has contributed to the implementation of in situ simulation,
using incident reporting and risk management to identify significant or
recurrent events, then using simulation to explore how these may have
17.
xiv About theauthors
occurred. This information can then be used to change policies or develop
the environment to prevent recurrence and reduce patient risk. With Jo‐Anne
Halliwell, he wrote ‘Enhancing patient safety through multidisciplinary in
situ simulation’ in Chapter 11.
Dr Kirsten Walthall MBChB MRCEM MSc(MedEd) PGCert is ST5 in
Emergency Medicine, North Western Deanery. She graduated from
Manchester Medical School in 2008 and obtained a PGCert (Merit) in
Leadership and Management (Healthcare) during FY2. After completing
ACCS, she took 2 years out of training to pursue her interest in medical educa-
tion and simulation, before returning to full‐time training in 2015. Kirsten has
developed simulation courses for emergency medicine trainees, run the simu-
lation competition at the Royal College of Emergency Medicine conference in
2015 and continues to deliver regular simulation‐based education. She com-
pleted her MSc (MedEd) with Merit in 2016. She wrote the section on social
media and simulation in Chapter 12. Her Twitter handle is: @K_Walthall.
James Wilson MBChB FRCA PGCE is a consultant anaesthetist with an
interest in regional anaesthesia and medical education. He has taught medi-
cal students from the beginning of his career and now teaches doctors and
allied health professionals across a variety of courses. His exposure to human
patient simulation started at medical school; this interest grew and led to a
medical education fellowship year at Lancashire Simulation Centre between
core and specialty training. He now teaches as faculty on a variety of simula-
tion‐based courses. Interests within SBME include human factors, video
feedback and analysis and predicting performance. He was lead author on
the section in Chapter 12 on ‘Using technology to facilitate effective feed-
back’ and Chapter 14 on ‘Training for simulation faculty’.
Sarah Wood MB ChB FRSC MA is a consultant in paediatric surgery at Alder
Hey Children’s Hospital in Liverpool. She has an interest in medical educa-
tion and simulation, facilitating both undergraduate and postgraduate teach-
ing and courses with a special interest in communication and debrief. She
was lead author on the section addressing ‘e‐learning and the flipped class-
room’ in Chapter 12.
18.
xv
Preface
Professor David Gaba,one of the pioneers of simulation training in healthcare,
observed in 1992, ‘… no industry in which human lives depend on the skilled
performance of responsible operators has waited for unequivocal proof of the
benefits of simulation before embracing it’. Fortunately, the evidence to sup-
port this worthy sentiment now exists in abundance and simulation training
for healthcare professionals is in widespread use.
The key educational theory underpinning the value of simulation training,
experiential learning, is far from a new concept, having been espoused in
ancient times by both Confucius and Aristotle but more recently by David A.
Kolb whose experiential learning cycle might have been specifically designed
with medical simulation in mind. Even without an understanding of these
formal educational principles, however, it is surely self‐evident that training
doctors, nurses and allied health professionals in a safe and supportive learn-
ing environment where they can practise without the risk of doing any harm
is a good idea – a view supported by data collected from patients and carers.
The authors cover experiential learning and allied theories in a complete
chapter of this book and helpfully point the reader to additional, more in‐
depth texts on these subjects.
I do not know anyone involved in simulation training who does not feel a
profound sense of reward and enjoyment in supporting learning in this envi-
ronment, but it is not easy. This book highlights very well the importance of
fastidious design of learning outcomes, careful preparation of the scenarios,
tools and technology and, most importantly, focused training in debriefing
skillsforfacultymembers.Acoretenetofexperientiallearningistherequirement
for reflective practice which is most effective when supported by facilitators
experienced in the use of what John Heron, in his Six‐Category Intervention
Analysis, would call ‘authoritative and facilitative interventions’ – learning
outcomes can so easily be jeopardised by the inexperienced debriefer.
We were, of course, using simulation in medicine long before the advent of
the technological advances which now support this training so effectively
19.
xvi Preface
and Ivery well remember practising the siting of epidurals using a simple
orange to give that distinctive feel of loss of resistance. However, colleagues
in the world of engineering and computer technology have opened up a
world of novel, cost‐effective and highly portable solutions to support simu-
lation training both in our education centres and in real clinical settings.
None of this training would be possible without the support of the resource-
ful and inventive simulation technologists in our centres. These are the inval-
uable team members who configure the AV systems to support debriefing,
programme a vast array of bespoke scenarios, reconfigure and repair increas-
ingly complex technologies and design innovative solutions to produce
bleeding into drains or the appearance of third‐degree burns on actors and
mannikins. We now have apps for iPhones and Android, wireless mannikins
and e‐learning platforms which provide extraordinary flexibility in the
development of innovative learning opportunities, all of which are explored
and signposted in this book.
The overarching purpose of simulation education is the transfer of
training received to the clinical workplace, i.e. to take the new or enhanced
skills back to the ward or operating theatre to improve the safety and care
of our patients. No practitioner of simulation‐based education would ever
say that simulation is the answer to all the challenges we face in medical
education but it is a very powerful adjunct to clinical apprenticeship and
deserves to be a cornerstone in the education of healthcare professionals
from all backgrounds. Simulation training can support the development of
competencies in both technical and non‐technical skills and plays a vital
part in enhancing the teamworking skills so essential in the management
of clinical crises. There is now clear evidence that regular crisis resource
management training incorporating simulation for multidisciplinary
teams in healthcare improves safety‐critical behaviours and, crucially,
patient outcomes, and Chapter 10 provides constructive direction in the
most effective use of simulation for safety training.
This book has been written by authors with a combined experience of over
50 years in simulation training for healthcare professionals. They have put
together a text that concisely covers all the aspects of the successful design
and organisation of simulation training, from the construction of scenarios
and use of the huge variety of technology to support simulation‐based educa-
tion to the design and operation of a simulation centre. How to Teach Using
Simulation in Healthcare joins the inventory of similar ‘How to’ titles from
Wiley at an opportune moment when time for training healthcare profes-
sionals is being compressed, as never before, by competing demands for ser-
vice delivery. This concise and pragmatic publication will be a welcome
20.
Preface xvii
support anduseful reference for experienced and novice educators in healthcare
who are using simulation to train healthcare professionals and I look forward
to many future editions.
Helen Higham MBChB, FRCA, SFHEA
Consultant Anaesthetist, Oxford University Hospitals NHS Foundation
Trust
Senior Clinical Research Fellow and Director of OxSTaR, University of
Oxford
President, ASPiH (2014–2017)
April 2017
2 How toTeach Using Simulation in Healthcare
looks at the human aspect of that process and explores the route to developing
expertise in managing the learning environment through faculty training.
Chapter 15 explores (albeit only in outline and with a somewhat cloudy
crystal ball) some direction of travel and supports a willingness to engage
with new possibilities as they emerge from changes in technology and orien-
tation as well as learner expectations.
We conclude with a short annotated bibliography describing books that
the team of authors have learned from over the years.
This book is largely the product of work initiated and sustained over a
number of years at Lancashire Teaching Hospitals NHS Foundation Trust
(hereafter LTHTR) at Royal Preston Hospital, where many of the writers and
editors work or have worked in the Lancashire Simulation Centre. We would
like to thank all learners and contributors to the programmes described in
this book, for their feedback and active participation in the various pro-
grammes, and our shared understanding of the processes. Specifically, we
would like to thank the following.
Anil Hormis, MBChB FCARCSI AFICM, Consultant in Anaesthesia,
Critical Care and Pre‐hospital Emergency Medicine, Rotherham NHS
Foundation Trust, for critical reading.
Karl Thies, MD FRCA DEAA FERC, Consultant Anaesthetist and Pre‐
hospital Emergency Medicine, Birmingham Children’s Hospital, who advised
on the European Trauma Course section in Chapter 11.
University of Manchester undergraduates, 2008 onwards.
University of Manchester SIFT funding.
Colleagues at Blackpool Teaching Hospitals NHS Foundation Trust.
Christine Davis and Steven Pettit gave helpful comments and corrections.
Additionally, those colleagues who have contributed to the varied pro-
grammes offered by the Simulation Centre.
Finally, we acknowledge the support of the LTHTR Workforce and
Education Directorate for continued funding and support.
Needless to say, all errors of omission and commission are the responsibility
of the editors.
Mike Davis
Jacky Hanson
Mike Dickinson
Lorna Lees
Mark Pimblett
4 How toTeach Using Simulation in Healthcare
appropriate education for a doctor. The curriculum was the basic sciences,
humanities and clinical studies initially, over 2 years. The Medical Act of
1886 stated that a graduate needed ‘the knowledge and skills requisite for the
efficient practice of medicine, surgery and midwifery’ (MacAlister, 1906). It
was Flexner’s reports of 1910 and 1912 that sealed the curriculum structure
of preclinical and clinical years over a 5‐year period (Cooke et al., 2006). This
was only removed from the Medical Act in the revisions of 1973 and 1983
(Cavenagh et al., 2011).
The knowledge of medicine expanded, and throughout the twentieth cen-
tury there have been concerns that the curriculum was overloaded and stu-
dents were not able to apply themselves or be ready for unsupervised clinical
practice. Sir George Pickering (1978) suggested the need to provide a cur-
riculum that allows the student to be able to weigh up evidence and reach a
decision, and found that students wanted their teachers to know how to
teach. Medicine had expanded so much that research was more important
than being taught how to teach. In 1993 the GMC published the report
Tomorrow’s Doctors, which recommended reducing the factual knowledge by
producing a core curriculum and developing special study modules, which
enabled students to develop critical thinking and reasoning. The authors
accepted that these ideas had been proposed before, but there were a number
of developments which provided the catalyst for these reforms, including
publications in the British Journal of Medical Education, documentaries on
television and the appointment of educators to medical schools. Prior to this,
very few people teaching medicine had any educational qualifications
(Cavenagh et al., 2011).
Jacky Hanson writes of her own student days:
In my experience as a medical student in the 1980s, very few of my pre-
clinical or clinical lecturers appeared to have any formal education in
teaching. The majority of teaching on the wards was by humiliation, but
there were some good teachers who stood out with a natural ability. As a
qualified doctor, I distinctly recall myself and a female colleague being
called Tweedle Dumb and Tweedle Dee by a senior surgeon who was
teaching us on the postgraduate Fellowship of the Royal College of
Surgeons course. (Hanson, 2012)
When did we get taught how to teach?
Before the 1990s, doctors were required to teach with no formal exposure to
either theory or practice. In 1957, the Association for the Study of Medical
Education (ASME) was formed by doctors interested in medical education,
26.
Simulation‐based medical education(SBME): some specifics 5
and they accepted non‐medical colleagues with educational expertise as
being capable of contributing to the process (Southgate, 2007). The
Association for Medical Education in Europe was founded in 1972 and both
these associations have been responsible for developing medical education
into a professional discipline. The first centre for medical education opened
in Dundee in 1975 (www.dundee.ac.uk/meded/aboutus/). More centres have
opened and it is now not uncommon for doctors to obtain a qualification in
medical education as well as insight into the needs of learners.
The Academy of Medical Educators (AoME) came into existence in 2006
and has made a significant contribution to both theory and practice of
medical education, providing leadership, promoting standards and support-
ing all those involved in medical education in a variety of contexts, including
simulation.
Specifically, within the context of SBME, the Association for Simulated
Practice in Healthcare (ASPiH) came into existence in 2009 as a product of
the amalgamation of the National Association of Medical Simulation and the
Clinical Skills Network, and is dedicated to providing support for the emerg-
ing simulation community.
All these organisations promote a thoughtful and evidence‐based approach
to medical education, and serve to illustrate the interest in medical education
by the community of healthcare professionals as a whole.
Where does simulation‐based medical education fit in?
Historically, medicine has been taught like an apprenticeship: you learn the
basic sciences, and then you are attached to different specialties to learn
about the application of that knowledge, and to learn more about dealing
with patients. As we will explore in Chapter 3, this knowledge is presented in
situations in context, i.e. on the ward seeing a patient and following what is
happening to that patient. Experience integrated the learning into a specific
context and culture, and involved specific activities. Learning to practise
medicine is learning in a social environment, which enables cognitive tools
to develop through social interaction. The more engaged a learner is, the
more is learned about medicine and its culture through the mechanisms
described as situated learning, in Chapter 3.
In contemporary medical education, various methods of educating medical
undergraduates and postgraduates have been developed, with simulation‐
based medical education (SBME) being one such modality. As we explore in
Chapter 3, simulation is the imitation of some real thing, state of affairs or
process. The act of simulating something generally entails representing certain
27.
6 How toTeach Using Simulation in Healthcare
key characteristics or behaviours of a selected physical or abstract system.
Simulation has been part of the medical education for years in its crude
form, as cadaveric dissection. From the time of Aristotle in 300BC, dissection
of corpses was used to gain insight into the function of the human body.
Leonardo da Vinci studied the circulation of blood and actions of the eye.
Simulation includes the reproduction of human systems to gain insight into
their function for performance optimisation, safety engineering, testing,
training and education. It can be used to show the eventual real effects of alter-
native conditions and courses of action. Simulation has improved to include
part task trainers such as IV access training with Resusci Annie for Basic Life
Support and the Heart Sim for Advanced Life Support. These are used purely
to practise specific skills and consolidate clinical guidelines in resuscitation.
The importance of simulation‐based medical education
The use of human patient simulators in north‐west England was first assessed
by Tony Gilbertson and Jacky Hanson in 2001, where they looked at simulation
across the nation. This report concluded that:
In our view the current climate of public opinion will no longer permit
medical practitioners to practise on patients when experience can easily
be gained in a clinical simulator. (Gilbertson Hanson, 2001)
Thus there was an ethical dilemma. Patients are not commodities to be practised
upon. The Hippocratic Oath states ‘First, do no harm’ but harm does occur
when training on patients, as mistakes do happen despite teachers monitor-
ing trainees. Patients have a right to decide on their own treatment, and that
includes whether they allow trainee doctors to do a procedure on them, pos-
sibly for the very first time. The era of ‘See one, do one, teach one’, once a
common experience, has ended.
Clinical simulation will have a place in the education of medical students,
junior doctors, specialist registrars, nurses and consultants. Simulators
should be made available … to protect patients from management of
critical conditions by inexperienced health professionals, to improve the
proficiency, confidence and morale of staff faced with these frightening
emergencies and to facilitate clinical governance by enabling health
authorities to be assured that staff are properly and regularly trained in
the management of emergencies, and that protocols for the management
for such emergencies in their hospitals are effective, realistic and applicable
to the local environment and the staff are fully familiar and can practise
and implement the protocols. (Gilbertson Hanson, 2001)
28.
Simulation‐based medical education(SBME): some specifics 7
Human patient simulation or whole body simulation allows the trainee to
practise to a higher level of competency prior to dealing with a real patient,
thereby reducing risks and potential harm.
Medical error and patient safety are playing an increasing part in medical
training. Brennan and his collaborators (1991) reviewed over 30000 admis-
sions to New York hospitals and found 3.7% adverse events overall, of which
58%wereduetopreventableclinicalerror,ofwhich13.6%died.Extrapolating
these figures and the Utah and Colorado figures to the whole of the USA sug-
gests that as many as 98000 Americans may die in hospital each year due to
medical error. The approximate cost of medical errors could be $17–29
billion. Wilson’s (1995) review of about 14000 admissions in New South Wales
hospitals in Australia showed that an adverse event occurred in 16.6% admis-
sions, of which 51% were preventable. In 13.7% of these cases, the adverse
event caused permanent disability and 4.9% resulted in death. When extrap-
olated to all Australian admissions, these data suggest up to 18000 deaths per
year, at an approximate cost of 4.7 billion Australian dollars (Wilson, 1995).
In the UK, Vincent and collaborators (2001) reviewed 1014 hospital
records, showing that adverse events occurred in 10.8% of patients, of which
48% were preventable. Clinical errors produced 6% permanent disability and
8% deaths. These findings were extrapolated to calculate the cost of extra bed
days of the adverse events, at approximately £1 billion. Investigation into
medical adverse events showed that 66% errors were due to human error or
non‐technical errors (DeAnda Gaba, 1991), very similar to figures obtained
in aviation (70–80%). The Confidential Enquiry into Maternal Deaths has
cited lack of teamwork and poor communication as major causes of sub-
standard care (Gibb, 1990). These reviews provide strong evidence that
SBME can be a very useful tool in medical education, allowing practice in a
safe environment and enabling medical personnel to practise as teams and
develop awareness of the non‐technical skills required for safe patient care.
The development of full body simulators started in the 1960s in the USA,
and has developed into very sophisticated systems which can be programmed
to respond to physiological and pharmacological changes. Over a number of
years, studies have been performed to look at the benefit and cost‐effective-
ness of simulators. These studies have shown a positive impact (Alinier et al.,
2006; Chopra et al., 1994; Gordon Powlowski, 2002). Weller and collabora-
tors (2004) looked at groups of medical students attending simulation work-
shops in medical emergencies, and the workshops were evaluated with
postcourse questionnaires. The study demonstrated that the students rated
the simulation sessions very highly, especially allowing them to utilise their
knowledge in a safe, realistic environment. In particular, they found simula-
tion helpful in the development of teamwork and a systematic approach to
29.
8 How toTeach Using Simulation in Healthcare
clinical problems. In another study, looking at simulation training with
nurses and doctors on acute medical emergencies, participants perceived
improvements in assessment diagnosis and treatment of these types of
patients. They also perceived improvement in their communication skills
(Hanson et al., 2004).
Aspects of simulation
Simulation has developed in medical education via a number of avenues:
• e‐learning for knowledge learning and updates – the flipped classroom
(see Chapter 12)
• computerised scenarios
• simulated patients, using actors as patients to develop communication
skills
• part task trainers to practise skills prior to doing the procedure on a patient
• (Advanced) Life Support courses to teach a systematic approach to treating
acute conditions
• virtual medical worlds that have been developed where working in a spe-
cific environment can be practised
• whole body simulation enables the combination of clinical scenarios, tech-
nical and non‐technical skills to be observed in situ within the clinical
environment.
All these aspects of simulation are used as adjuncts to lectures, tutorials,
problem‐based learning, consolidating knowledge, technical skills and drill
training, and provide an insight into non‐technical skills (human factors) for
multidisciplinary groups.
An example of the approach is described below.
Lancashire Simulation Centre
The Lancashire Simulation Centre specialises in whole body simulation
using video debriefing, and a team comprising Jacky Hanson, Mark Pimblett,
Mike Dickinson and Graham Jones have been engaged in developing a pro-
gramme of undergraduate and postgraduate exposure since 2009.
Initial simulations now strike us as crude, and they have become more
sophisticated through experience and with new technological developments
in both mannikin design and software availability. This was enhanced by the
foresight of the Undergraduate Department in providing a purpose‐built sim-
ulation centre, equipped with two simulation rooms, an integrated debriefing
room and control room. Our initial funding, which is vital as equipment is
expensive, was from the Undergraduate Department from the University of
Manchester, so initially we concentrated our efforts on undergraduate
30.
Simulation‐based medical education(SBME): some specifics 9
students. Some may have said that simulation is an expensive commodity to
use with undergraduates but we disagree. It has provided added value to the
curriculum and highlighted the non‐technical skills
students need to develop
to improve patient safety. We have formalised the integration into the curricu-
lum by setting scenarios within each module, initially in the third year with a
Heart‐Lungs‐Blood module, extending into the fourth year with obstetrics,
gynaecology, paediatrics and orthopaedics and continuing with the final year
revision sessions. This is explored in more detail in Chapter 11.
All scenarios cover specific learning outcomes, both technical and non‐
technical, and are mapped to NHS learning outcomes. With the passport for
practice at the end of the fifth year, we provide bleep sessions, in which the
students are given a bleep for the day and are intermittently bleeped to the
simulation centre, to perform a number of tasks. These might include filling
in a drug chart, seeing a patient or prioritising several jobs on the wards, and
highlight workload management, situation awareness and decision making.
More recently, in conjunction with colleagues from the Department of
Educational Research at Lancaster University, as part of a Knowledge Transfer
Partnership, we have been developing a blended learning programme. This
utilises on-line learning about the subject prior to attending the simulation and
debrief. These learning modules reinforce the clinical knowledge required to
maximise the potential of the simulation session (Shahoumian et al. 2014a, b).
The Foundation Years training programme utilises simulation to cover
specific scenarios commonly seen in the wards and most of the learning
comes from non‐technical skills, especially communication over the phone.
Various courses have been designed to provide specific skills, for example
• airway management for non‐anesthetists;
• ventilation respiratory care course for physiotherapists;
• training for respiratory nurses in non‐invasive ventilation;
• multidisciplinary training looking at non‐technical skills;
• training in non‐technical skills for specialist trainees and consultants in
orthopaedics, plastics and general surgery, anaesthetics, emergency medicine,
and obstetrics and gynaecology using specific behavioural markers for each
specialty;
• training for transfer;
• theatre training.
All these courses, to a greater or lesser extent, highlight individuals’ non‐
technical skills, which can be categorised into four main domains:
• leadership
• teamwork or followership
• decision making
• situation awareness.
31.
10 How toTeach Using Simulation in Healthcare
In these domains, communication and how we think are vital in prevent-
ing error and determining the causes of errors in cognition. Some specialties
have taken the non‐technical skills further and developed behavioural mark-
ers specific to those specialties. All these domains are required in clinical
work and so we use a generic format for undergraduates.
As we explore in Chapter 3, clinicians and allied professionals are explor-
ing the multidisciplinary environment within a model of situated learning in
which clinical encounters are replicated in the simulation laboratory. These
can be videoed and individual feedback provided. The development of digi-
tal video and specific software for individual and team analysis in sport has
provided SBME with a method of reinforcing the debrief session which takes
place after the clinical scenario has ended. The Lancashire Simulation Centre
have developed a matrix marking system, currently being validated, to pro-
vide digital video tagging to capture team and individual performances
(Quinn et al., 2012). This has enriched the debrief sessions with a powerful
instant reminder of individual and/or team behaviour, which can be explored
further and provides insight into attitudes and behaviour in the clinical
environment.
Conclusion
This chapter has provided an explanation of how medical education has
developed to accommodate the vast increase in knowledge base that is
expected to be learned during the 5‐year training period for medicine. It has
explored the development of doctors trained in medical education and the
concept behind the development of simulation‐based medical education,
and its role in the future. Chapter 3 will go on to provide some educational
theory that may apply to SBME.
References
Alinier G, Hunt B, Gordon R Harwood C (2006) Effectiveness of intermediate
fidelity simulation training technology in undergraduate medical education.
Journal of Advanced Nursing, 54(3), 359–369.
Brennan TA, Leape, LL, Laird MN, et al. (1991) Incidence of adverse events and
negligence in hospitalized patients: Results of the Harvard medical practice study 1.
New England Journal of Medicine, 324(6), 370–376.
Cavenagh P, Leinster S Miles S (eds) The Changing Face of Medical Education.
London: Radcliffe.
32.
Simulation‐based medical education(SBME): some specifics 11
Chopra V, Gesink BJ, de Jong J, Bovill JG, Spierdijk J Brand R (1994) Does training
in the anaesthetic simulator lead to improvement in performance? British Journal of
Anaesthesia, 73, 293–297.
Cooke M, Irby DM Sullivan W (2006) American medical education 100 years after
the Flexner report. New England Journal of Medicine, 355(13), 1339–1344.
DeAnda A Gaba DM (1991) Role of experience in the response to simulated critical
incidents. Anesthesia and Analgesia, 72(3), 308–315.
General Medical Council (1993) Tomorrow’s Doctors. London: GMC.
Gibb D (1990) Confidential enquiry in to maternal death. International Journal of
Obstetrics and Gynecology, 97(2), 97–99.
Gilbertson T. Hanson JM (2001) Report for the NHS Executive (North West).
Manchester, UK: Education and Training Directorate on Human Patient Simulation
(HUPAS)
Gordon JA Powlowski J (2002) Education on‐demand: the development of a simu-
lator based medical education service. Academic Medicine, 77(7), 751–752.
Hanson JM (2012) A clinician’s thoughts in simulation in medical education. AACE
Conference, Montreal, Canada, December 21.
Hanson JM, Smith C, Luthra P, Cutting P, Pimblett M Zahir M (2004) An assess-
ment of the educational value of the Laerdal SimMan in improving the assessment
and treatment of critically ill patients. 10th International Conference of Emergency
Medicine, Cairns, Australia, June 6–10.
MacAlister D (1906) Introductory Address on the General Medical Council and Its
Work. Manchester: Manchester University Press.
Nutton V Porter R (eds) (1995) The History of Medical Education in Britain.
Amsterdam: Rodopi.
Pickering G (1978) The Quest for Excellence in Medical Education. Oxford: Oxford
University Press.
Quinn A, Wilson J, Pimblett M, Dickinson M Hanson J (2012) Validating the
matrix marking system for NHS simulation‐based medical education assess-
ment. In: Bastiaens T Marks G (eds) Proceedings of E‐Learn: World Conference
on E‐Learning in Corporate, Government, Healthcare, and Higher Education 2012.
Chesapeake, VA: Association for the Advancement of Computing in Education.
Available at: www.learntechlib.org/p/41687 (accessed 3 April 2017).
Reinarz J (2005) Towards a history of medical education in provincial England. In:
Nutton V Porter R (eds) The History of Medical Education in Britain. Amsterdam:
Rodopi, pp. 30–37.
Shahoumain A, Saunders M, Zenios M, Parchoma G Hanson J (2014a) Blended
simulation based medical education: a complex learning/training opportunity. In:
Proceedings of a Conference on Learning and Collaboration Technologies:
Technology‐Rich Environments for Learning and Collaboration. Switzerland:
Springer.
Shahoumian A, Parchoma G Hanson M (2014b) Blended simulation based medical
education: a durable network for learning? Network Learning Conference,
Edinburgh.
33.
12 How toTeach Using Simulation in Healthcare
Southgate L (2007) A History of ASME: 1957–2007. Available at: www.asme.org.uk/
images/HISTORY_book_inner.pdf (accessed 3 April 2017).
Vincent C, Neale G Woloshynowych M (2001) Adverse events in British hospitals:
preliminary retrospective record review. British Medical Journal, 322, 517–519.
Weller J, Robinson B, Larsen P Caldwell C (2004) Simulation based training to
improve acute care skills in medical undergraduates. New Zealand Medical Journal,
117(1204), 1119–1127.
Wilson RM (1995) The quality in Australian health care study. Medical Journal of
Australia, 163, 458–471.
14 How toTeach Using Simulation in Healthcare
design and the novel use of technology. The first of these is explored more
fully in Chapter 7 and the latter in Chapter 12.
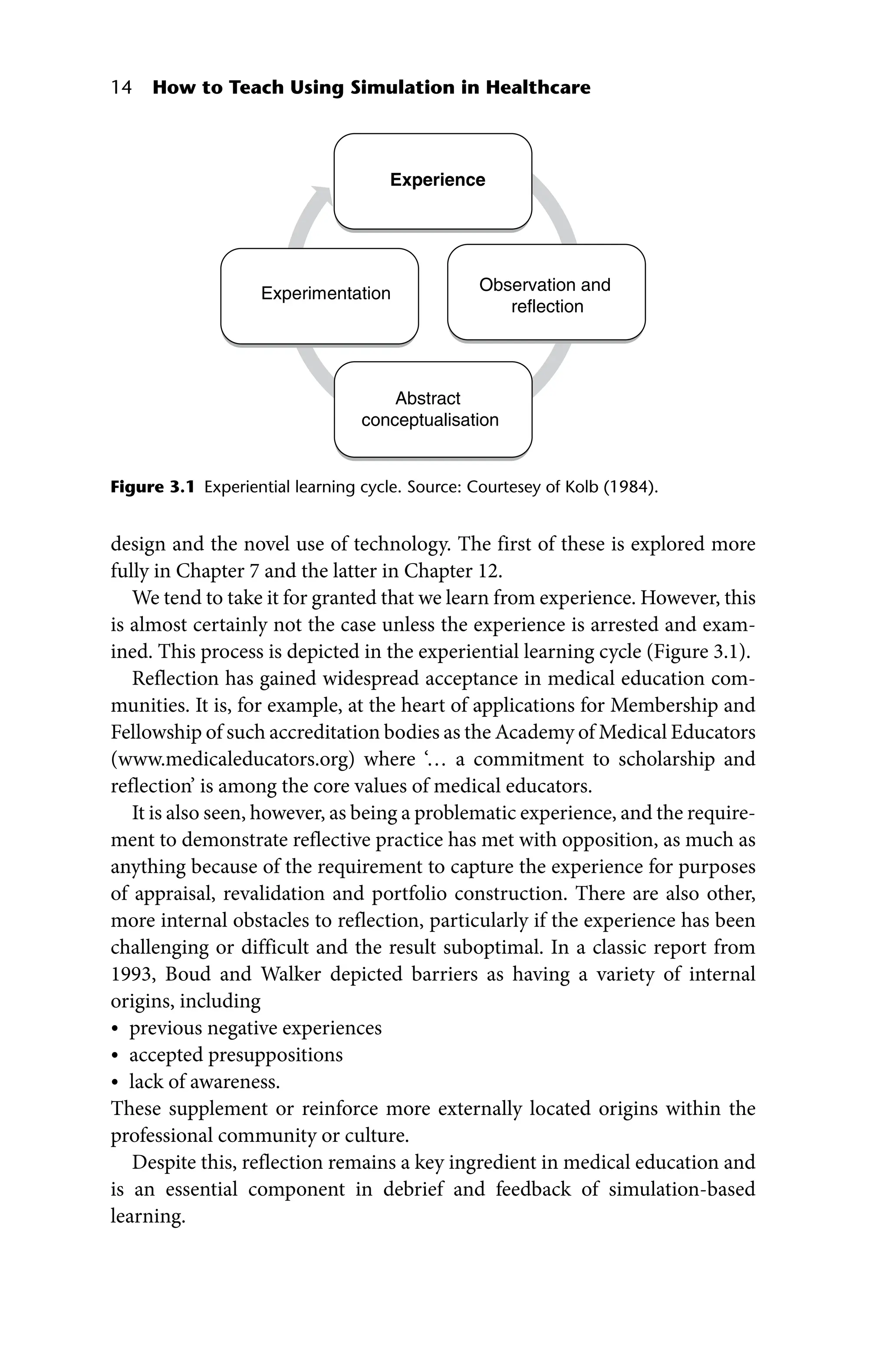
We tend to take it for granted that we learn from experience. However, this
is almost certainly not the case unless the experience is arrested and exam-
ined. This process is depicted in the experiential learning cycle (Figure 3.1).
Reflection has gained widespread acceptance in medical education com-
munities. It is, for example, at the heart of applications for Membership and
Fellowship of such accreditation bodies as the Academy of Medical Educators
(www.medicaleducators.org) where ‘… a commitment to scholarship and
reflection’ is among the core values of medical educators.
It is also seen, however, as being a problematic experience, and the require-
ment to demonstrate reflective practice has met with opposition, as much as
anything because of the requirement to capture the experience for purposes
of appraisal, revalidation and portfolio construction. There are also other,
more internal obstacles to reflection, particularly if the experience has been
challenging or difficult and the result suboptimal. In a classic report from
1993, Boud and Walker depicted barriers as having a variety of internal
origins, including
• previous negative experiences
• accepted presuppositions
• lack of awareness.
These supplement or reinforce more externally located origins within the
professional community or culture.
Despite this, reflection remains a key ingredient in medical education and
is an essential component in debrief and feedback of simulation‐based
learning.
Experience
Observation and
reflection
Abstract
conceptualisation
Experimentation
Figure 3.1 Experiential learning cycle. Source: Courtesey of Kolb (1984).
36.
Simulation in (medical)education: some background 15
The question we now address is how simulation fits into the ‘experience’ of
the experiential learning cycle. Simulation belongs to a tradition based on
the ‘fiction contract’ (Deickmann et al., 2007) or the notion of the ‘willing
suspension of disbelief’ (Coleridge 1817/1991), and while it is true that
it contains elements of these, we consider that it is firmly embedded in an
experience of reality.
Jones explores the difficulty of reaching an adequate definition of
simulations.
In my first book (Jones 1980) I criticised existing definitions and expressed
a preference for descriptions. But I added, ‘If a short definition is really
necessary, perhaps it might be “Simulations are reality”.’ … In my second
book (Jones 1982a) I devised the following definition of an educational
simulation:‘Realityoffunctioninasimulatedandstructuredenvironment’…
Today I might ask for a little more space, and say something like:
‘A
simulation in education is an untaught event in which sufficient
information is provided to allow the participants to achieve reality of
function in a simulated environment.’ (Jones, 1987, pp. 118–119)
This notion of ‘reality’ is one to which we will return in a number of chapters
because an understanding of it, and its importance in the nature of the learn-
ers’ experiences, is a key ingredient in the success or otherwise of the simula-
tion event.
John Lanchester described the notion of the willing suspension of disbelief
in terms of our experience of reading a novel in these terms:
All fiction depends on what Samuel Taylor Coleridge called ‘the willing
suspension of disbelief’, the reader’s decision to put the argumentative,
quibbling part of his mind into neutral and go along for the narrative
ride. The suspension is voluntary, though not necessarily conscious;
it’s not as if you reach up and toggle a setting in your brain. Rather, as
readers, we usually fight the story a little bit at the beginning, while we’re
getting our ear in; then we submit, and are carried along by the flow,
unless something happens to jolt us out of it. If something makes our
disbelief become unsuspended – one implausibility too many, a series of
narratorial bum notes – then the whole fiction comes crashing down.
(Lanchester, 2016)
You may recognise this from your own experience both as a reader of
novels,
but also as a participant in possibly low‐fidelity simulations (for example, in
Basic Life Support).
Whatever the precise definition, ‘experience’ is the key ingredient here,
something described by Hall and Wooster as a situation where:
37.
16 How toTeach Using Simulation in Healthcare
Ideas are formed and reformed through experience. They are not fixed
and immutable. Learning is a process in which concepts are derived from
experience and constantly modified by experience (and in describing the
work of Kolb that) … the learner is torn between opposing ways of
dealing with the world. Striving to observe openly and to reflect from
several perspectives, she works to create new concepts and integrate
knowledge with theories she already holds, and then to use these theories
in the
solution of new problems. (Hall Wooster, 1984)
The nature of the simulation experience can provide a challenge to fidelity,
given that it is based in the notion of using an object in order to represent the
‘real world’. In working within simulation, learners are expected to buy into
the reality and experience the pressures as if the simulation was a real‐world
event. Some of this is a product of reaction to equipment and the clinical
scenario, i.e. physical realism, and this is something that is sought in high‐
fidelity simulations. Alternatively, it is the product of the psychological state
that arises when a group of learners are put in a situation of cognitive stress.
The buy‐in, therefore, is a product as much of learner perception and cogni-
tive load as it is of the ‘reality’ of a plastic mannikin. This will be explored in
more detail in Chapter 5.
Simulation and the real world
As we have explored, simulation can be seen as having the capacity to imitate
aspects of the clinical environment, even using low‐fidelity equipment with-
out putting patients at risk. Scenarios can be varied in complexity and
adjusted to maximise relevance, as follows:
• Learning is driven and best presented through realistic and complex prob-
lems that allow learners to learn to think and practise like experts in the field.
• Content is learned through activities that help solve those problems.
• The facilitator role moves from providing and structuring information and
knowledge, to enabling ‘real‐life’ problem solving (the sage on the stage to
guide on the side).
• The environment must support active engagement, discussion, evaluation
and reflective thinking within a collaborative environment (based on
Vincini, 2003).
While not stress free (stress is an inevitable feature of the experience), it lacks
the consequences of error or hesitation that might arise in the resuscitation
room or on the ward. Furthermore, it is a teaching event and is designed to
improved knowledge, skills and affect. As is often claimed:
Simulation has been developed to provide a highly valid replication of the
clinical environment. (Bradley Postlethwaite, 2003)
38.
Simulation in (medical)education: some background 17
While there are some reservations that can be attached to this claim, there
is, nevertheless, widespread agreement among simulation participants on the
highlevelsofsatisfactionabouttheirexperience.ArecentstudyofManchester
undergraduate students’ experience at the LTHTR (Davis Hanson, 2015)
reported that simulation
• improved confidence levels (85% increased somewhat)
• was beneficial to clinical training (100%)
• provided positive experience (100%).
Typical comments included the following:
• I found my first simulation to be very informative. I think it is a useful
and innovative tool that is great for introducing medical students to an
environment where they are expected to manage patients for real.
• … I found the session very helpful, and quite fun.
• … I found the experience extremely stimulating and a great opportunity to
put skills into practice in a safe environment.
• I really enjoyed the simulation, I’m excited for the next one, and I can see
why it’s such a good way of learning. I also value the security of going through
a scenario where it’s impossible to do anything dangerous to a patient.
This is, however, a perspective that arises from an understandable naivety and
lack of experience, and is in stark contrast to the observation made on a recent
course attended by mainly ex‐military paramedics who considered simulation
as ‘playing with plastic dummies’. This may, however, reflect the military
approach to simulation (see Davis et al. 2008) and to experience in the field.
In seeking to come up with a form of words that adequately represent the
complexity of the cognitive processes within the simplicity of the setting,
therefore, a more thorough rubric emerged.
Where the cognitive load is high and when students are prepared to buy
into the magic of simulation … total fidelity is of minor importance. The
magic does not trick us, it makes us believe. Participants can do this if:
• they suspend disbelief, and
• their brains are busy.
(based on email between Davis and Norris, 2013)
This is an important issue and one which is the basis of continued confidence
in an educational process that gives such an immediate and risk‐free (to
patients) experience of clinical practice.
Role play – an aside
Almost by definition, simulation involves a degree of role play, given that
the ‘actors’ are playing a role, rather than managing a case on the ward or in
the ED.
39.
18 How toTeach Using Simulation in Healthcare
Part of the challenge for psychological reality, explored in more detail in
Chapter 5, is the relationship of the learner to the idea of role playing, and
this is worth some attention.
Role play can involve any of the following:
• a person playing themselves in a familiar situation
• a person playing another in a familiar situation
• a person playing themselves in an unfamiliar situation
• a person playing another in an unfamiliar situation.
In the most psychologically real environment, the modality of choice is
the first of these, i.e. a person playing themselves in a familiar situation.
While this could be mundane, it is also a safe starting place for learners at the
beginning of their exposure to the complexities of managing a clinical case.
As they become more confident, on the basis of successful management of
familiar cases, they can move on to playing themselves in an unfamiliar
situation.
It is rare that learners are put in a situation where they are playing in either
of the other two modalities. In much low‐ to medium‐fidelity simulation in,
for instance, life support course scenarios, experienced instructors may be
asked to perform as another in a familiar situation (e.g. an experienced
faculty member may role play an inexperienced junior doctor managing an
airway in a trauma scenario). The purpose of this is to provide the learner
managing the scenario with the need to provide adequate support, guidance
and prompting in the face of a less confident candidate.
When thought of in the way outlined above, role play can become much
less threatening.
Situated learning
In much of formal, traditional education, there is an assumption that learn-
ing is an individual effort. Learning takes place in the heads of individuals
and from time to time, attempts are made to assess how much learning has
taken place. This is a very powerful model which has implications for teach-
ing at all levels of education. However, much of our learning takes place
within a social context and is accordingly the consequence of negotiated
meaning and understanding. Effective adult education and continuing
medical education (CME) attempt to come closer to more informal meth-
ods of learning, in which learners interact with the world and try to make
sense of it. When this is done with other learners, it becomes social con-
structivism, whereby learners interact with one another as well as their
environment.
40.
Simulation in (medical)education: some background 19
ThisderivesinpartfromattemptsbytheRussianpsychologist LevVygotsky
(1896–1934) to explain what happens when children learn language. This
theory was re‐examined and developed further in 1991 by Lave and Wenger,
who called it situated learning, and it is considered to have a number of char-
acteristics that are significant for the way in which
work‐based learning and,
by association, simulation impact on the learner experience. These are
• zone of proximal development
• scaffolding
• legitimate peripheral participation
• cognitive apprenticeship
• activity theory
• communities of practice.
Zone of proximal development (ZPD)
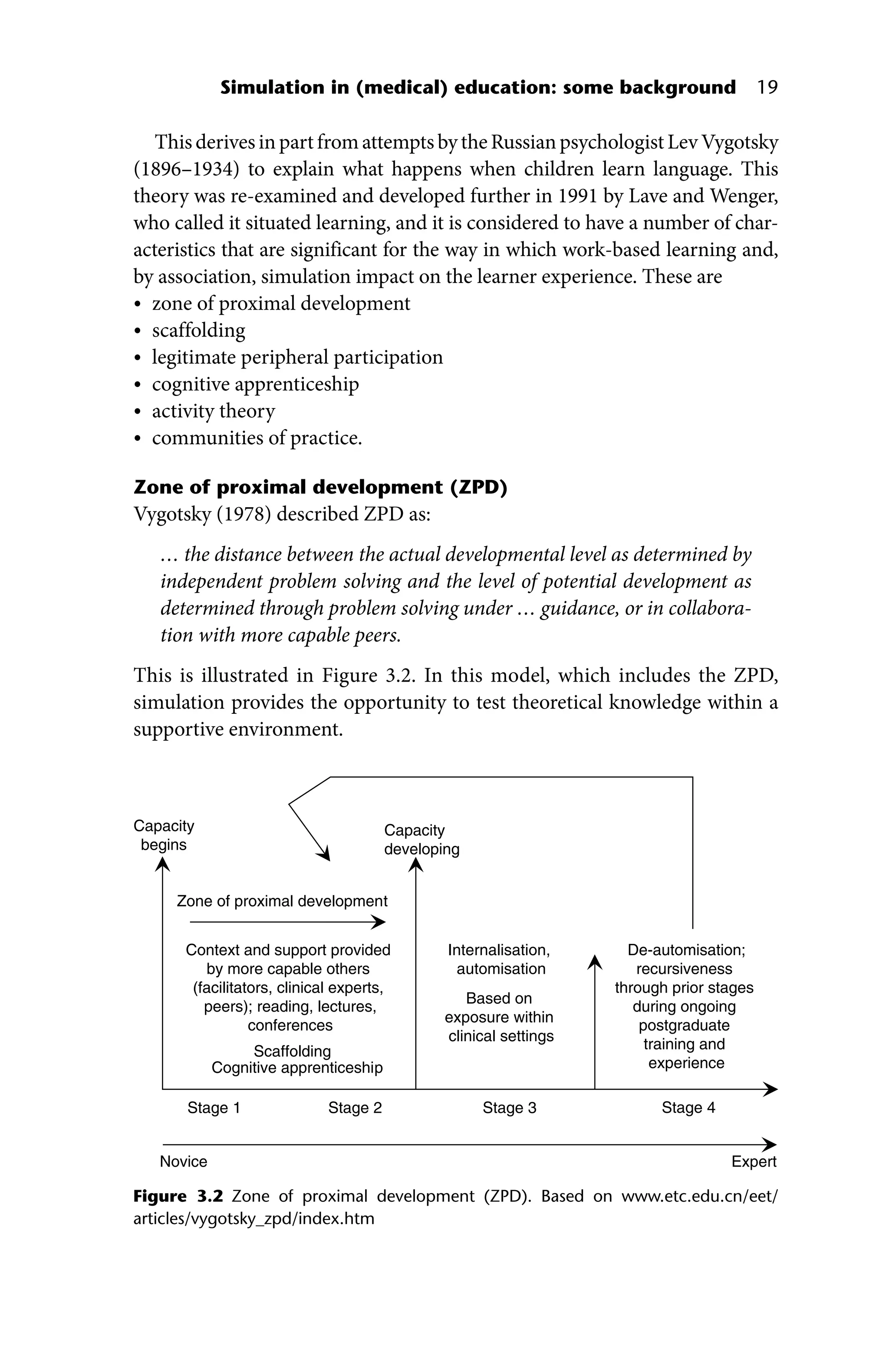
Vygotsky (1978) described ZPD as:
… the distance between the actual developmental level as determined by
independent problem solving and the level of potential development as
determined through problem solving under … guidance, or in collabora-
tion with more capable peers.
This is illustrated in Figure 3.2. In this model, which includes the ZPD,
simulation provides the opportunity to test theoretical knowledge within a
supportive environment.
Zone of proximal development
Context and support provided
by more capable others
(facilitators, clinical experts,
peers); reading, lectures,
conferences
Scaffolding
Cognitive apprenticeship
Capacity
begins
Capacity
developing
De-automisation;
recursiveness
through prior stages
during ongoing
postgraduate
training and
experience
Internalisation,
automisation
Based on
exposure within
clinical settings
Novice Expert
Stage 1 Stage 3
Stage 2 Stage 4
Figure 3.2 Zone of proximal development (ZPD). Based on www.etc.edu.cn/eet/
articles/vygotsky_zpd/index.htm
41.
20 How toTeach Using Simulation in Healthcare
Scaffolding
Scaffolding contributes towards learners’ development. As depicted above,
learners are dependent on other members of the community for ‘assistance’
(including expert insight when appropriate) as they come to terms with pat-
terns of social interaction, specific language and ways of behaving. Along with
these social phenomena, they draw on pre‐existing knowledge (arising from
presimulation VLE packages, previous exposure in clinical settings – see
Chapter 12), specific skills (supported by skills laboratory experiences) and
appropriate affect. Among these elements, Lave and Wenger (1991) argue that
the experience gives them insight (albeit tacit) of all the elements of case man-
agement, including the patient, relatives, artefacts and other clinicians of varied
skill. This process in development during stage 1 is referred to as ‘scaffolding’.
Responsibility for learning passes from the teacher to the learner as the
learner demonstrates competence. Scaffolding, therefore, can be seen as an
infrastructure of information, either from prior knowledge or through
teacher input, to which new material from the world can be anchored. It can
involve any of the following:
• models
• cues
• prompts
• hints
• partial solutions
• think‐aloud modelling
• direct instruction.
It also serves to
• provide clear direction
• reduce learners’ confusion
• clarify purpose
• keep learners on task
• clarify expectations
• incorporate assessment and feedback
• point learners to worthwhile sources
• reduce uncertainty, surprise and disappointment.
Some of this emerges from the interactions within stage 1 (i.e. a simulation)
and others are features of stage 2 (i.e. formal teaching through lectures, semi-
nars, private reading, etc.) that may be taking place simultaneously (although
not necessarily in concert with particular simulations).
Legitimate peripheral participation
Lave and Wenger (1991) wrote that learning is ‘a process of participation …
that is at first legitimately peripheral but that increases gradually in engagement
and complexity’.
from him arenow growing freely in the stoves of the Glasgow
Botanic Garden. They appear different from the one figured and
described by St. Hilaire, from the south of Brazil, and will, I suspect,
prove to be a distinct, though nearly related species. Leaving the
garden, we walked a little way into the country, where I hoped to
meet with something more interesting; and in this expectation I was
not disappointed, as many new plants were added to my collections.
On the dry bushy hills in this neighbourhood a wild fruit-tree grows
very plentifully; it is the Mangába of the Brazilians, and the
Hancornia speciosa of botanists; it is a small tree belonging to the
Natural Order Apocyneæ, the small leaves and drooping branches of
which give it somewhat the resemblance of the weeping birch. The
fruit is about the size of a large plum, of a yellow colour, but
streaked a little with red on one side, and the flavour is most
delicious.
In the afternoon we returned to Olinda, to dine with another
gentleman to whom I also carried letters, Senhor da Cunha. He had
been educated in England, and was an intelligent man. After dinner
we walked out to see the town, which is very pleasantly situated on
an eminence not far from the sea. It is a place of considerable size,
and in the olden time must have been a stirring one, particularly as
regards the clergy, judging from the number of churches, convents,
monasteries, c. It has now, however, a deserted and desolate
appearance, many fine houses being untenanted and falling to
decay, and the streets are grown over with grass and weeds. On the
outskirts of the seaward side of the town, there are the ruins of a
large monastery, which we went to see on account of a hermit who
had lived there upwards of seventeen years. We found it to be a
very large building, consisting of a church in the centre, still in use,
and two wings, containing the apartments formerly inhabited by the
friars, which are fast running into decay, particularly those in the
south wing. The north wing is in much better repair, having a few
good rooms, which are inhabited by some of the students attending
a theological and medical school, established in Olinda. Along the
corridors, and in some of the larger rooms, are still a few paintings,
44.
but in astate of much decay. While surveying this great fabric, we
could not help thinking of the contrast it now offers to the times, not
long gone by, when its walls re-echoed to the footsteps and prayers
of the devotees of a religion, which was then in a much more
flourishing state than it now is, over nearly the whole of the empire
of Brazil.
It was among the ruins of the south wing that the hermit lived.
We visited the room in which he was said to be generally found, but
he was not there. We then passed through a small court nearly
choked with rubbish, and entered a large dark room, partly filled
with old bricks and lime. Upon the floor of this wretched apartment
we found him lying, presenting a most miserable appearance. His
only covering consisted of a piece of thin black cloth wrapped round
his body, his head, arms, legs, and feet being bare. He appeared to
be about sixty years of age, but his long grey hair and beard made
him look older, perhaps, than he really was. He was moaning and
otherwise seemed to be in great agony, and it was with some
difficulty he told us that two days before, while walking across the
floor of the room above, it gave way, and he was precipitated to the
place where we found him extended, and from which he was unable
to move. We tried to raise him, but the slightest movement gave him
excruciating pain. As some of his bones seemed to be broken, a
young man who had accompanied us, went off immediately to
procure assistance, and have him taken to the hospital. All the
information I could obtain relating to this unfortunate being, was
that at one time, he had been an officer in the army, and was now
doing penance for a murder he had committed in his youth. We also
visited a convent, the nuns belonging to which prepare preserved
fruits for sale. Unlike the one I visited at Bahia, we could only speak
to, not see, those who were within. The fruit was put upon a shelf of
a revolving kind of cupboard, and in this manner sent out to us; the
money and empty plates were returned in the same way. Like all the
preserves I have met with in the country, those we had here were
spoiled with too much sugar.
45.
For the firstfew days, my walks did not extend much beyond the
suburbs of the town. The country being quite flat, the soil sandy,
and the dry season having commenced, the herbaceous vegetation
in the more exposed situations was beginning to suffer for want of
rain. For many miles round the town, the Cocoa-nut and other large
Palms grow in the greatest profusion, mixed with fine trees of the
Cashew-nut, then loaded with their curious and refreshing fruit of a
yellow or reddish colour, and the Jack, the Bread-fruit, and the
Orange. Much attention, I observed, is paid to the gardens attached
to the houses near the town, many of them being tastefully laid out,
and adorned with beautiful shrubs, partly Brazilian and partly of
Indian origin. The Mimosa and other hedges, as about Rio, are
festooned with climbers, among which the Cow-itch plant
(Stizolobium urens) is the most abundant. There is also in many
places a large species of Dodder (Cuscuta), which climbs over the
hedges with its long yellow cord-like branches, and gives them a
most singular appearance. The sea-coast yielded me many curious
plants, particularly one part of it about eight miles to the southward
of the town, where the soil for some distance inland is very sandy
and covered with shrubs. There I found in great plenty a new kind of
those curious mossy Cacti (Melocactus depressus, Hook.); it was but
a small one, being only about four inches high, and eighteen in
circumference.
About a fortnight after my arrival at Pernambuco, Dr. Loudon
removed to his country house, situated on the banks of the Rio
Capibaribe, about four miles west from Recife; and, as the country
round it was chiefly uncultivated, this afforded more ample scope for
my researches. The Rio Capibaribe, which empties itself into the
harbour at the Recife, is of small size, and is navigable only for
canoes to a distance of about ten miles from the town. The
navigation for six miles, as far as Monteiro, is very pleasant, and the
scenery is rendered more agreeable by the number of villas,
surrounded by gardens, which are scattered along its banks. Many of
these houses are inhabited during the fine or dry season only, when
most of the wealthy citizens resort to them for the benefit of bathing
46.
in the river;for, in hot climates, fresh water is preferred, as bathing
in salt water generally produces great irritation on the surface of the
body, from the salt crystallizing there, unless washed off with fresh
water. For the purpose of bathing, each house has a large shed
projecting into the river, the tops and sides of which are covered
with cocoa-nut leaves. They are mostly rebuilt every year, as they
are generally carried away by the floods in the rainy season.
About twenty miles to the westward of Pernambuco, there is a
small German Colony called Catucá; it was established about
eighteen years before, at a period when a German regiment, which
had been in the service of the Brazilian government, was here
disbanded, but it is now fast dwindling into decay. The few families
residing there gained a livelihood by the manufacture of charcoal,
which they carried to town for sale. Being desirous of spending a
day or two at this place, I started early one morning in the
beginning of November, accompanied by Mr. White, a young
gentleman whom I had previously met on the Organ mountains. We
were guided by two Germans who were returning from Pernambuco,
and their horses carried our luggage. Our route for about two hours
was through a flat country, principally planted with mandiocca,
although a great part of it was still uncleared, only the large trees
having been cut down: a few of those remaining rose high above
their fellows of the wood, and agreeably diversified the landscape.
After passing through this cultivated country, and ascending a slight
eminence, we entered the virgin forest. Previously the road had
been of a sandy nature, but now we found it to consist of hard red
clay. Many of the trees were very lofty, although they do not
commonly attain the stature of those in the Province of Rio, nor
have their trunks the same circumference. Among the shrubs that
grew below them, I observed a few Melastomaceæ, Myrtaceæ, and
Rubiaceæ. Here everything betokened a drier atmosphere, and a
more arid soil than at Rio. There were no Ferns, Begonias, Pipers, or
Orchidaceous plants. On the stems and branches of the larger trees
a few Bromeliaceæ and Aroideæ were alone to be seen. After riding
for about an hour through this forest, we reached the cleared valley
47.
containing the cottagesof the colonists, several of which we passed
before reaching the one in which we remained. These cottages are
generally of small size, although much superior in cleanliness and
neatness of arrangement to those belonging to the same class of
Brazilians. At night we slung our hammocks in a small apartment,
and enjoyed a sound sleep till morning.
My friend being desirous of having a few days’ shooting in the
woods with one of the Germans, I determined to accompany them,
in the hope of making some additions to my botanical stores. We set
off early, entering the wood about a mile from the cottage. Here, as
in similar situations near the town, I observed a great deficiency of
herbaceous vegetation, and in a walk of about two hours collected
only a few Ferns. In passing through this wood, we saw an
enormously large tree, a species of Lecythis; the ground beneath it
was covered with its curious pot-like capsules nearly as large as a
man’s head, their resemblance to a pot being much increased by the
large lid which falls off from the top of each when the seeds within
are ripe. Most of those we saw were empty, the nuts having been
taken out by the monkeys, who are very fond of them. Leaving this
wood, we suddenly came upon another cleared valley, containing the
ruins of several cottages; this, we were told, had been the first site
of the settlement, but as the colonists were forbidden to cut any
more wood in that direction, they moved their quarters to the place
before mentioned. Near these dismantled dwellings we found
abundance of pine-apples, and refreshed ourselves with some which
were ripe, sheltering ourselves from the sun under the shade of an
out-house which had formerly served as a place for the preparation
of farinha from the Mandiocca root. Near this place I found two
beautiful trees, one of them a species of Vochysia, covered with long
spikes of bright yellow flowers, and the other the splendid
Moronobea coccinea, literally covered with its globular crimson
blossoms. In returning I collected specimens of a yellow-flowered
Palicourea, called Mata Rato, not, however, the same plant which is
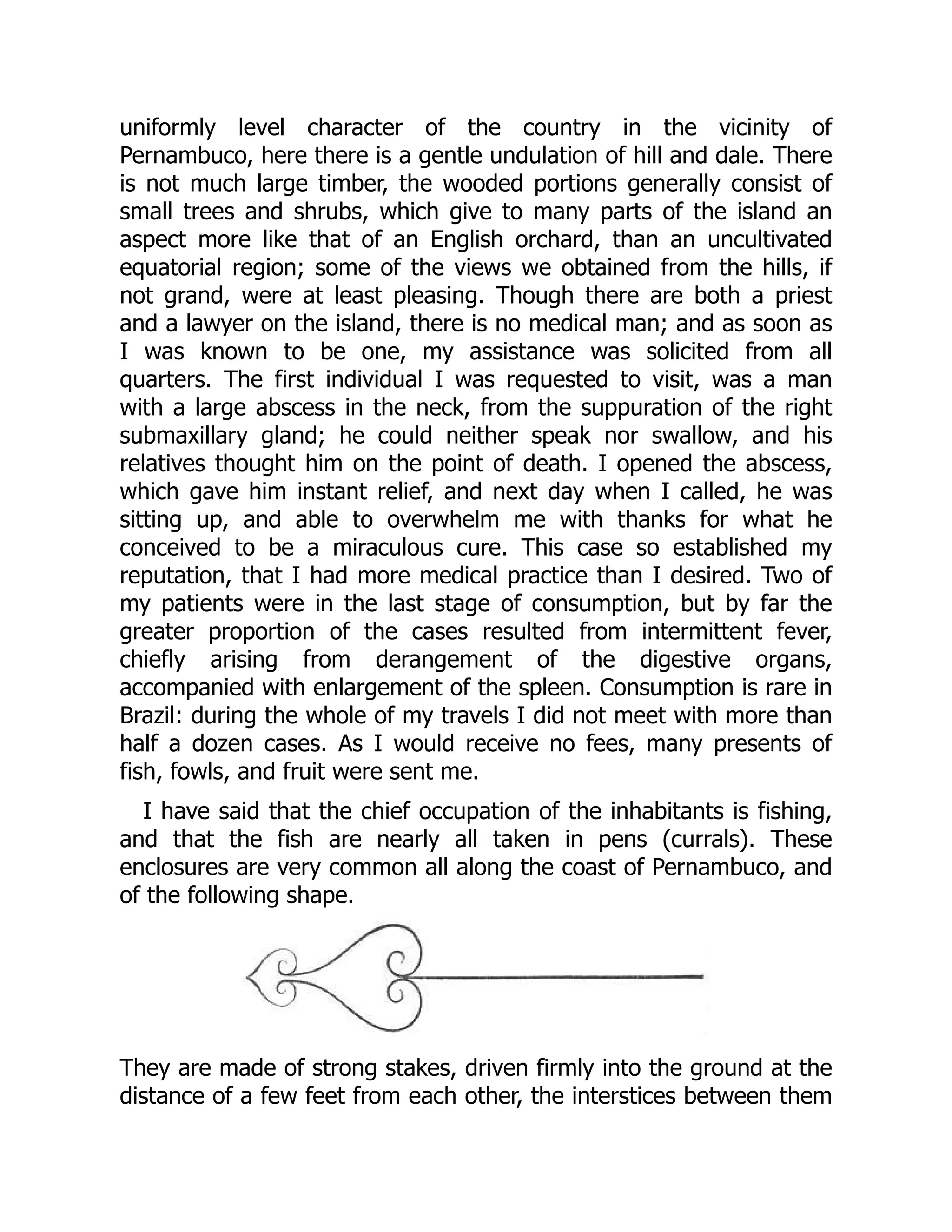
known at Rio by the name of Erva do Rato. It proves,
48.
notwithstanding, that poisonousqualities are attributed to different
plants of the same genus in different parts of the country.
Close to the main land, and about thirty miles north from
Pernambuco, there is a small island called Itamaricá, which on
account of its fine climate and soil, and the abundance and
superiority of the fruit produced there, is designated the garden of
Pernambuco. I was desirous of visiting this place before leaving the
province, and with this intention I started about the middle of
December, and considered myself fortunate in having as a
companion Mr. Adamson, a young gentleman who had been some
years in the country, and was fond of botanical pursuits. To make
the voyage, we had to hire a Jangada, one of the raft boats so
common on this part of the coast; it was manned by a crew of three
men. To a stranger it appears a very singular kind of craft, and had I
not been well assured that, primitive as their construction seems,
they are perfectly safe, I should have felt some hesitation in
embarking on one of them.
Having got our luggage properly placed on its elevated platform,
so as to be out of the reach of the water, which continually washes
over these rafts, we commenced our voyage. The wind almost
constantly blows at that season from the north-east, and
consequently was nearly right against us, rendering it necessary to
beat up between the reef and the shore; the intermediate distance
varying from a quarter of a mile to two miles, all the way from Recife
to the island. By four o’clock in the afternoon, finding that the
unfavourable wind prevented our performing more than half the
voyage, we determined to land at a small fishing village called Pao
Amarello, and there pass the night. It was not without some
difficulty that we obtained a shelter wherein we could sling our
hammocks; after meeting with several refusals, the owner of a small
public-house (Venda) pointed out an empty hut made of cocoa-nut
leaves, and permitted us to take possession of it for the night.
Hither, therefore, we moved our luggage, and after a supper of
stewed fish and farinha, slept soundly till daybreak. After getting up,
we took a walk a little way into the country; the soil we found to be
49.
sandy, and theherbaceous vegetation completely scorched up by
the drought. At this place the reef is about a mile distant from the
shore, and is distinctly perceptible along its whole line, both at high
and low water, for although the ebb tide leaves the rocks quite bare,
the surf marks its position even at the highest flow. The wind having
now shifted more to the eastward, we were enabled after breakfast
to proceed on our voyage, and as we made much more rapid
progress than on the preceding day, we reached the island at noon,
and landed on the eastern side of it at Pilar, the principal town.
We carried with us two or three letters of introduction, and the
first we delivered obtained us quarters. The name of our host was
Alexander Alcantará, the proprietor of a large salt-work, of which
there are several on the island. His house, like nearly all the others
we saw, was of one story, the walls consisting of a frame-work of
wood, the interstices of which were filled up with a kind of clay, and
the roof was covered with tiles; there were four good rooms in it, all
floored with boards; it was delightfully situated near the sea, and
surrounded by cocoa-nut trees. In the afternoon we were taken by
our host to see his salt-works, which were established in a valley
into which the tide flows at high water. The water from which the
salt is made, is kept in large reservoirs, whence it is from time to
time made to flow into pits, where it is allowed to evaporate. At this
place, which is called Jaguaribe, there are twenty-four distinct
manufactories, belonging to as many individuals. The place where
the water is evaporated is divided into small compartments,
measuring sixteen feet by twelve. In that belonging to Senhor
Alcantará, there are one hundred and twenty such compartments;
into each of these, two inches of water is allowed to flow from the
large reservoir, and in eight days this is completely evaporated. It
yields him, altogether, annually, about four hundred alqueires of salt,
each alqueire weighing eight arrobas, and each arroba thirty-two
pounds. Three qualities are produced, the best being used for
domestic purposes, a middle sort for curing fish and an inferior kind
used principally to salt hides. On an average it brings about 2s. 6d.
an alqueire, so that his whole income from this source is only about
50.
50l. a year.Besides the manufactories at this place, there are others
in different parts of the island.
The island, which is separated from the main land by a strait
about half a league broad, is nearly three leagues in length, and
from one and a half to two in breadth. It contains only two small
villages, viz., Itamaricá, situated on a height near the sea, on the
south-east side, containing only about twenty houses; and Pilar, the
place at which we landed, formed of a few irregular streets, and
containing about eighty habitations. The whole number of houses in
the island, we were told, amounted to three hundred, and the entire
population to about two thousand. Although there are many very
comfortable looking dwellings, yet the mass of the houses have a
poor appearance, being either formed of wicker-work and mud, or of
cocoa-nut leaves. As fishing is the principal occupation of the
inhabitants, their houses are generally near the shore. The fish are
mostly taken in pens (currals) that are constructed of stakes a little
beyond low-water mark. Another source of income to the
inhabitants, is the cocoa-nut trees, which form a dense deep belt
round the upper part of the island; both the fish and nuts are taken
to Pernambuco for sale. In the interior of the island there are three
sugar plantations; and several of the more wealthy of the
inhabitants cultivate grapes and mangoes to a considerable extent,
both of which sell well in Pernambuco, bringing a better price than
those cultivated elsewhere in the province. Good grapes I bought at
tenpence a pound, but they give the cultivator a great deal of
trouble, as the vines are sure to be attacked by a large brown ant,
and stripped of their leaves in a single night, unless care be taken to
have the lower part of the stem isolated by water. The whole of the
province of Pernambuco is much overrun by these insects. During
the time of our visit the mangoes were just getting into season, and
I found them to be very much superior in flavour to any I had
previously tasted; they are much smaller than those cultivated near
Pernambuco, and very much resemble peaches in colour.
During the few days we remained on the island we made many
excursions through it in all directions; instead of the almost
51.
uniformly level characterof the country in the vicinity of
Pernambuco, here there is a gentle undulation of hill and dale. There
is not much large timber, the wooded portions generally consist of
small trees and shrubs, which give to many parts of the island an
aspect more like that of an English orchard, than an uncultivated
equatorial region; some of the views we obtained from the hills, if
not grand, were at least pleasing. Though there are both a priest
and a lawyer on the island, there is no medical man; and as soon as
I was known to be one, my assistance was solicited from all
quarters. The first individual I was requested to visit, was a man
with a large abscess in the neck, from the suppuration of the right
submaxillary gland; he could neither speak nor swallow, and his
relatives thought him on the point of death. I opened the abscess,
which gave him instant relief, and next day when I called, he was
sitting up, and able to overwhelm me with thanks for what he
conceived to be a miraculous cure. This case so established my
reputation, that I had more medical practice than I desired. Two of
my patients were in the last stage of consumption, but by far the
greater proportion of the cases resulted from intermittent fever,
chiefly arising from derangement of the digestive organs,
accompanied with enlargement of the spleen. Consumption is rare in
Brazil: during the whole of my travels I did not meet with more than
half a dozen cases. As I would receive no fees, many presents of
fish, fowls, and fruit were sent me.
I have said that the chief occupation of the inhabitants is fishing,
and that the fish are nearly all taken in pens (currals). These
enclosures are very common all along the coast of Pernambuco, and
of the following shape.
They are made of strong stakes, driven firmly into the ground at the
distance of a few feet from each other, the interstices between them
52.
being afterwards filledup by small straight rods closely tied together.
The straight line of rods is sometimes nearly a quarter of a mile in
length, and runs out away from the shore; it answers the purpose of
guiding the fish into the enclosures at the farthest end of it.
The day before we left the island, we accompanied our host to
visit the curral belonging to him, in order to witness the method of
taking fish; they are only visited at low water. We went in a canoe to
the entrance of the innermost enclosure; our host then stripped
himself, as did also another person who accompanied us, and
entered the inner enclosure, taking with them a small net a little
deeper than the water, with a short pole fixed to each end of it. One
of the men then fixed one of the poles perpendicularly close to one
side of the entrance to the enclosure, while the other began to
unfold the net, closing with it the entrance so as to prevent the
escape of the fish; he then walked round by the side of the
enclosure till he reached the other person, when the net was rolled
up, thus enclosing in it all the fish contained in the curral, which
amounted to about a dozen very fine ones. We were informed that
at this season very few are taken; so few, indeed, that they are
scarcely sufficient for the consumption of the families to whom the
currals belong; in the rainy season, however, they are taken so
abundantly, that boat-loads of them are sent to the Pernambuco
market. We returned to Recife in a large canoe.
The Author’s Motivefor this Excursion—Voyage to the Southward—Description of the Coast
and Observations on the great Restinga—Reaches Barra de S. Antonio Grande—Arrives
at Maceio—Description of the Town and surrounding Country—Resolves to visit the Rio
S. Francisco—Embarks in a Jangada and coasts to the Southward—Batel—Lands at
Peba—Journey thence to Piassabassú on the Rio San Francisco—Ascends the River to
Penêdo—The Town Described—Productions of the District—Its Population—Voyage up
the River—Mode of Navigation—Arrives at Propihà—Vegetation of the Country—
Description of a Market Fair—Dress of the People—Voyage continued to Traipú—Passes
the Ilha dos Prazeres—Barra de Panêma—Abundance of Fish of the Salmon Tribe—
Village of Lagoa Funda—Island of S. Pedro—Its Indian Population described—Continues
the Voyage—Fearful Storm—Return to S. Pedro—Serious Illness and Detention there—
Scarcity of Food—Renounces in consequence all intention of proceeding further—
Returns to Penêdo—Scheme for Navigating the Rio San Francisco—Reason why it never
will succeed—Arrives again at Maceio—Visits Alagoas—That City Described—Leaves
Maceio—Coasting Voyage—Singular Mode of catching Fish—Return to Pernambuco.
The great object of my visit to the north of Brazil was to make a
journey from the coast to the high lands which lie on the eastern
side of the Rio Tocantins. This part of the country, which I was
strongly recommended to visit by Von Martius and others, on
account of its botanical riches, is distant from Pernambuco about
1,200 miles, and nearly directly west from it. Although I was
desirous to begin this journey I was advised by persons well
acquainted with the interior of the country not to undertake it
towards the end of the rainy season, on account of the difficulty of
finding grass and water for the horses after the period when every
thing has been scorched up by the burning sun of the dry season.
Nor is the period of the rains less exceptionable for the undertaking
of a long journey, since, during the four months which it generally
lasts, there are scarcely two consecutive dry days. It was now about
the end of January, and as the period of my entering upon my
proposed expedition would not be sooner than the end of June or
beginning of July, to pass the intervening time I determined to visit
Maceio, a small seaport town in the province of Alagoas, about half-
way between Pernambuco and Bahia; and from thence to make an
excursion to the Rio San Francisco, and, if possible, up that river to
the great falls of Paulo Affonço. As no other conveyance was to be
55.
had for Maceio,I was obliged to take a passage in a canoe which
was going down laden with goods.
It was about three o’clock in the afternoon of the 30th of January,
1838, before I could obtain my passport, upon which I immediately
embarked, and after undergoing the necessary examination at a
custom-house boat, we got outside the reef, and ran down before
the north-east trade-wind till seven o’clock p.m., when we came to an
anchor for the night, in a small sandy bay about four leagues to the
south of Pernambuco. During the passage, we several times ran foul
of the stakes of fishing pens, which are common along the coast. I
may here describe the nature and appearance of the craft in which I
was embarked; it was about forty feet long and three feet broad,
being the trunk of a large tree hollowed out; a few feet at each end
of it were decked over, and the little cabins so formed were filled
with parcels and provisions; when empty they served as sleeping
berths for the crew, which consisted of the master and two men. It
had a single, long, slender mast, to which a triangular sail was fixed,
the lower part of which was stretched out by a long boom; a little
below the gunwale on each side were lashed two logs of light
buoyant wood, nearly as long as the canoe, of the same kind of
which jangadas are made; while these enable her to carry more
cargo, they serve also to prevent her from upsetting, and give a
place to walk upon, as the cargo, in our vessel, rose two feet above
the body of the canoe. It may well be imagined that there was but
little comfort in such a conveyance, as I was obliged to sit constantly
upon one of my trunks, with no other shelter from the sun and rain
than that afforded by an umbrella. On the shore, close to where we
anchored, two large fires were burning, by the light of which we saw
several people and three or four huts. I was anxious to land here, to
obtain, if possible, a place to sleep on, but the master said he would
not go on shore, as he was not on good terms with some of the
inhabitants, and did not choose to risk himself among them. After
supping, therefore, with the crew on oranges, farinha, and boiled
salt-fish, I wrapped myself in my poncho, and lay down on my
trunks, and slept, but certainly not comfortably, till morning. At dawn
56.
of day weagain got under way, and about eight a.m., passed Cape
St. Augustino, a rocky point, behind which the land rises from one to
two hundred feet above the level of the sea; this is eight leagues to
the south of Pernambuco, the intervening country being one
continued flat. During the whole of the day we ran down very close
to the shore, always keeping between it and the reef. The country is
of an undulating hilly nature, wooded with small verdant trees and
shrubs, many of the latter covered with flowers. The beauty of the
coast, although a little monotonous, was, notwithstanding, some
recompense for a day of continued exposure to the sun. At eight
o’clock in the evening we again came to an anchor, at a place where
the master was well known; here we landed, and I found that my
quarters for the night were to be a smith’s work-shop; next day,
however, I ascertained that it was the best house in the place, being
formed of wicker-work and mud, while the others were composed of
stakes and cocoa-nut leaves. The following morning the master of
the canoe took me to the house of a relation, about two miles
further along the shore, where we met with a kind reception. As
some of the cargo of the canoe had to be landed here, and more
taken in, we remained here all day, which I did not regret, as it
rained heavily till night; on this account I was prevented from
making an excursion into the country, although I did not perhaps
lose much, as, in one short walk, I found nearly the whole
herbaceous vegetation burnt up. The land here rises higher than at
any other place between Pernambuco and Maceio, the faces of
several low hills, exhibiting a kind of coarse grained sandstone rock,
exactly of the same nature as the reef which runs for several
hundred miles along the coast both to the north and south of
Pernambuco. This reef, which is covered with small shells and
coralloid substances, Mr. Darwin supposes either to have been
formed by a bar of sand and pebbles formerly existing below the
water, which was first consolidated, and then elevated; or by a long
spit of sand, running parallel to the coast, having had its central part
consolidated, and afterwards, by a slight change in the set of
currents, having the loose matter removed, so as only to leave the
hard nucleus. Neither of these suppositions, I feel fully satisfied,
57.
accounts for theorigin of the reef, because, at the place where we
now were, I could trace, at low water, a rocky connection between
the reef and the rocks of which the hills were composed. It is more
probable that the reef owes its origin to the decay of the rock
between it and the shore, but in what manner I will not attempt to
explain. This sandstone, as I will hereafter show, belongs to the
lower series of the chalk formation.
We slept at the house of the relation of the master of the canoe,
who was a tailor by trade, and an acknowledged poet and wit: in the
society of whom and his family, consisting of several sons and
daughters, the time passed away most agreeably. Early in the
morning of the following day we again pursued our voyage, keeping,
as before, close along the shore, and at about two o’clock p.m., we
arrived at Barra de S. Antonio Grande, a small village about nine
leagues to the north of Maceio, consisting of about one hundred
houses, the greater part of which are made of cocoa-nut leaves, and
are mostly situated on a projecting point of flat land, bounded on
one side by the sea, and on the other by a small river of the same
name as the village, both deriving their appellation from a large bar
of white sand which stretches across the mouth of the river at some
distance from the shore. The inhabitants live principally by fishing,
but I was informed on my arrival at Maceio, that it is a place much
resorted to by slave vessels for the delivery of their cargoes, and it
certainly appears to be well suited for such a purpose.
In the afternoon I took a walk a little way along the banks of the
river, but did not find much to interest me; like all other sandy parts
along the coast, the vegetation here consists of low shrubs mixed
with a few small trees; Schinus terebinthifolius being by far the most
common. One of the most striking vegetable productions near the
village is a large wild fig-tree growing close to the river, beneath the
shade of which four large canoes, larger than the one in which I
arrived, were being constructed; this also forms a rendezvous for the
gossips of the village, who assemble there in the afternoon, beneath
its wide-spreading branches which reach nearly to the ground, thus
shading them from the sun. The leaves of the tree are about six
58.
inches long andthree broad, with fruit about the size of a large
gooseberry. In the evening I strolled through the village, and found
that nearly all the inhabitants had turned out of their houses to
enjoy the beautiful moonlight and the delightfully cool evening
breeze; many of them were squatted on the bare ground, some
were lounging on mats, while others were stretched out on cocoa-
nut leaves. In most of these groups, one or more of the individuals,
generally young men, were amusing the others by playing lively airs
on the guitar. As the master of the canoe belonged to the village, I
was invited to sleep at his house, but as he could not afford me a
bed, I was obliged to repose on a hide in the corner of a small room;
scarcely, however, had I fallen asleep when I was awakened by
legions of hungry bugs, that came pouring out from the cracks in the
mud walls; unable to endure this torment I got up, and taking-the
materials which formed my bed outside the house, I shook them
well, and spreading them in the open air, I slept there comfortably
till morning. This was the only time during the whole of my travels
that I was annoyed to any extent by this insect, which is not nearly
so common, or so abundant as the flea.
Next day, Feb. 4th, we left Barra de San Antonio Grande about
mid-day, and reached Maceio at five o’clock in the evening. Shortly
afterwards I delivered the letters of introduction I had brought with
me from Pernambuco to Mr. Burnet, the only British merchant in the
place, who kindly invited me to remain with him during my stay. The
town of Maceio is of considerable size, containing about 5,000
inhabitants; previous to the independence of Brazil, when the
Portuguese were expelled by the Brazilians, the population
amounted to upwards of 7,000, and as these were the principal
capitalists, the trade of the place has declined considerably ever
since. The town itself stands on a platform about fifty or sixty feet
above the level of the sea, and distant from it about a quarter of a
mile; but at a little more than a mile to the north-east, there is a
small village called Jaragua, close to the sea, where there are two
wharfs for the loading and unloading of goods, and a custom-house.
The bay of Maceio is of considerable size, forming a kind of
59.
semicircle, and offeringgood anchorage for shipping. Formerly much
cotton and sugar were shipped from this port in British bottoms, but
now scarcely more than two or three English vessels visit it in the
course of the year, the greater part of this produce being sent either
to Bahia or Pernambuco. The country round Maceio is not so
monotonous and flat as that around Pernambuco; low undulating
ridges of hills reaching close to the sea, covered with a vegetation of
low trees and shrubs. During several walks which I took in the
vicinity, in company with a young Scotchman who had been
sometime resident there as a medical practitioner, I made many
additions to my botanical collections, particularly on a flat sandy
tract to the north-east of the town. Among these I may mention a
fine Diospyros, a curious Eriocaulon, Marcetia taxifolia, an
Eschweilera different from that found at Pernambuco, and a
Melocactus. Maceio is considered more unhealthy than Pernambuco
or Bahia, ague being of very frequent occurrence, particularly at the
beginning of the rainy season.
The Rio San Francisco being only thirty-two leagues to the
southward of Maceio, and learning that it was navigable, without
interruption, for upwards of a hundred miles, I resolved to visit it. A
Portuguese gentleman, however, to whom I was directed for
information on the subject, having, a few years before, made the
voyage up to the great falls (Cachoeira de Paulo Affonço), informed
me that as it was then the season at which the river rises to its
greatest height, the head waters being far to the south, he would
not advise me to undertake the voyage, in consequence of the
dangerous navigation at the period of the floods, as well as from the
little chance there would be of my adding much to my collection,
from the dried up state in which I should find the vegetation, owing
to the long continued drought. Still I determined to go, as nothing
better presented itself to pass the time, and hitherto, moreover, I
had always found the difficulties of travelling much less than they
were represented to be. I considered myself fortunate in being able
to hire, as a servant, the black who accompanied the gentleman
above alluded to.
60.
Having made thenecessary preparations for the voyage, I
engaged a jangada to take me along the coast to the mouth of the
river, and left Maceio at five o’clock a.m., on the morning of the 15th
of February. I intended to leave at eleven o’clock the night before, at
the rising of the moon, but when I reached the beach with my
luggage, the owner of the jangada was nowhere to be found,
although he had faithfully promised to be waiting for me. I
immediately sent Pedro, my black servant, in search of him, who
soon afterwards returned unsuccessful; and I had no resource but to
walk backwards and forwards on the beach till shortly before five
o’clock in the morning, when he made his appearance. On
questioning him about his absence, he told me with the greatest
coolness, that as I did not arrive exactly when the moon rose, he
thought I should not come till morning, and that, in order to pass
the time, he had gone out to fish. Having at length embarked, we
soon lost sight of Maceio under the influence of a strong north-east
wind, and, coasting along a flat shrubby shore, we arrived at night
at the mouth of a small river, on the south bank of which, about a
mile up, there is a little village called Batel. At this place, which is
twenty leagues distant from Maceio, we remained for the night. I
preferred sleeping in the jangada to one of the small cocoa-nut-leaf
cottages that was offered to me, but I had reason to repent of
having done so. It was full tide when we arrived at the village, and
the jangada was brought close to the shore, so that when the tide
ebbed it was left dry. I did not then recollect that all muddy shores
covered with mangroves, particularly at the mouths of rivers,
abound with mosquitos, but I was soon reminded of the fact by
being awoke about midnight with my face and hands smarting and
swollen from the bites of those annoying insects. As I slept in my
clothes without any covering, I was obliged to shield my face with
my pocket-handkerchief, and thrust my hands into my pockets.
Although I was thus in some measure protected from their bites, it
was long before I could again fall asleep, from the continued
humming noise, almost as loud as that of bees, which they were
making around me. When I got up at daybreak, after a restless
night, I found that besides the mosquitos, I was surrounded by
61.
thousands of asmall black sand-fly (Merohy), not much larger than
a grain of fine gunpowder, but whose bites are no less irritating than
those of their larger congeners. The morning tide, we found, did not
rise so high as it did on the previous evening, and it was with some
difficulty that the jangada was floated into deep water, which was
not effected till nearly nine o’clock, a.m. In crossing the bar at the
mouth of the river, we had to pass through a line of small breakers,
three of which swept over the elevated platform on which I was
sitting, and drenched me to the skin, thereby rendering the
remainder of the voyage very uncomfortable. It was one o’clock,
p.m., when we reached a little village called Peba, which is situated
on the coast, about five leagues to the north of the mouth of the Rio
San Francisco: this was the termination of my sea-voyage, as the
heavy surf which breaks over the shallow bar of that river will not
allow jangadas to enter it. The village is situated a little way inland,
and is hidden from the sea by a high embankment of sand, which at
this place is very much drifted by the wind; it is, however,
recognised at a considerable distance, from the number of tall
cocoa-nut trees which grow near the shore. I was here particularly
struck with a fact which goes a great way to explain the
phenomenon of the stem of a fossil tree being found passing
through several strata of sandstone rock. Many of the cocoa-nut
trees have their stems embedded to the depth of fifty feet and
upwards in the embankment of sand which stretches along the
shore, and in many places is several hundred feet broad; some of
them, indeed, are so deeply embedded, that the nuts can be
gathered without climbing the tree. Now as this sand has
accumulated at different periods, particularly during the prevalence
of the north-east trade-wind, it must present, if ever it becomes
hardened, a vast number of irregularly horizontal beds, through
which the stems of the palms will be found to pass.
From a fisherman, whom I met on the shore, I obtained
permission to occupy an empty hut till the next day. While seated on
the trunk of a tree, which was lying on the beach at high-water
mark, I observed that on the shore here, as well as along the coast,
62.
crabs of varioussizes abounded; and, as I had to wait until my
luggage was landed and carried to the hut, I amused myself by
watching the operations of a small species, belonging to the genus
Gelasimus that was either making or enlarging its burrow in the
sand. About once in every two minutes it came up to the surface
with a quantity of sand enclosed in its left claw, which, by a sudden
jerk, it ejected to the distance of about six inches, always taking
care to vary the direction in which it was thrown, so as to prevent its
accumulation in one place. Having a few small shells belonging to a
species of Turbo in one of my jacket pockets, I endeavoured to
throw one of these into its hole, in order to see whether it would
bring it up again or not; of the four that were thus thrown, one only
entered the hole, the others remaining within a few inches of it. It
was about five minutes before the animal again made its
appearance, bringing with it the shell which had gone down, and
carrying it to the distance of about a foot from its burrow, it there
deposited it. Seeing the others lying near the mouth of the hole, it
immediately carried them, one by one, to the place where the first
had been laid down, and then returned to its former labour of
carrying up sand. It was impossible not to conclude that the actions
of this little creature, which holds so low a station in the chain of
beings, were the result of reason, rather than of blind instinct by
which the actions of the inferior animals are generally thought to be
guided, for man himself, under the same circumstances, could not
have acted with more judgment.
On the day following our arrival at Peba, I made arrangements
with the owner of an ox-cart to take me with my luggage to
Piassabassú, a little village situated on the north bank of the Rio San
Francisco, and about two leagues distant from its mouth. He
promised to come early in the forenoon, but, much to my
annoyance, did not make his appearance till five o’clock in the
afternoon, shortly after which we started. We kept along the sandy
shore for about two miles, then went a little inland and continued
our route in a direction nearly parallel to the shore through a flat,
sandy, bushy country, in which Mouriria Guianensis, Aubl., and
63.
several species ofLauraceæ, were very abundant. It was indeed
dark during the greater part of the journey, but on my return I had
ample opportunity of observing the nature of the vegetation. I was
not at all sorry, after we had once started, that we had been thus
delayed, as travelling in this country is far more pleasant in the
evening than during the heat of the day. Our cart was of a very
primitive construction, similar to that seen everywhere in the interior
of Brazil, and little different from that used by the Romans. It
consisted of a rude frame, supported on two wheels about five feet
in diameter, constructed of solid plank; and was drawn by six oxen,
yoked in pairs, goaded on by two drivers, each carrying a slender
pole about ten feet long. One of the drivers goes before to lead the
way, while the other urges on the oxen with his long pole. The axles
are never greased, and the creaking noise they continually make,
which we heard at a great distance, is most disagreeable; the reason
given for not greasing them is, that the cattle are so accustomed to
the noise that they would not go on without it. It was ten o’clock at
night when we arrived at the end of our journey, and as there was
no place where a stranger could put up, and being without
introduction to any resident in the village, I was taken by our
conductor to the house of one of his acquaintances, where the only
accommodation to be obtained was in a small and very dirty
apartment in the hut, which did not much signify, as I slept in my
own hammock.
Piassabassú is a small village, where the greater part of the
houses surround a large square with a church in its centre; these are
nearly all of one story, and, being white-washed on the outside, they
present a cleanly appearance. Many of those situated nearest to the
river, were abandoned on account of its flooded state, being then
higher than it had been since the year 1793, when the inundation
reached to a still greater height. On the morning after our arrival at
this place I hired a canoe to convey me to the Villa do Penêdo,
seven leagues further up the river. We started at eleven o’clock, a.m.,
but the current was so strong that the canoe was obliged to keep
close along shore to be able to make way against it; a small sail, by
64.
which we werepropelled, was often barely sufficient to keep us from
being carried downwards; at such times our two men were forced to
use their paddles. At Piassabassú the river is about two leagues
broad, but the opposite side cannot be seen on account of a large
island which stands in the middle of the stream; it was only after we
had proceeded upwards about half a league, that I first saw the
whole breadth of this magnificent river. The country, for about three
leagues, is flat on both sides, which the present flood had inundated
to a considerable extent. We passed large fields of sugar-cane,
where nothing was to be seen but the tops of the leaves, which,
waving in the stream, gave them the appearance of verdant
meadows; where trees existed, nothing but their upper branches
were visible, and almost every house that we passed had only its
roof appearing above the water. The river begins to rise in the
month of October, which is the commencement of the rainy season
in the southern provinces, the sources of its origin, and continues to
do so until the end of March. At about five leagues from the coast,
the country, on the south side of the river, slightly rises, and from
thence to Penêdo it is of an undulating character, but the opposite
side still continues flat. After pursuing our course upwards about two
leagues on the north, we crossed over to the southern bank, in
order to obtain advantage of the breeze. A few sugar plantations
exist on both sides, but the vacancies in the forests made by the
cultivated spots are scarcely apparent. By the force of the stream,
particularly in certain turns of the river, the banks were greatly
encroached upon by a continual process of undermining, and we
saw great masses of earth falling in, the trees which grew thereon
being floated down by the current. We did not come in sight of
Penêdo till within a league of it, when, turning round a high rocky
wooded point on the south side, the white houses were seen brightly
lighted up by the rays of the sun, which was then just setting nearly
opposite to the town. Shortly afterwards we distinguished Villa Nova,
a small town situated about half a league below Penêdo, but on the
south side of the river. As the Rio San Francisco divides the province
of Alagoas from that of Sergipe, it will be seen that the Villa do
Penêdo is in the former, while Villa Nova is in the latter.