

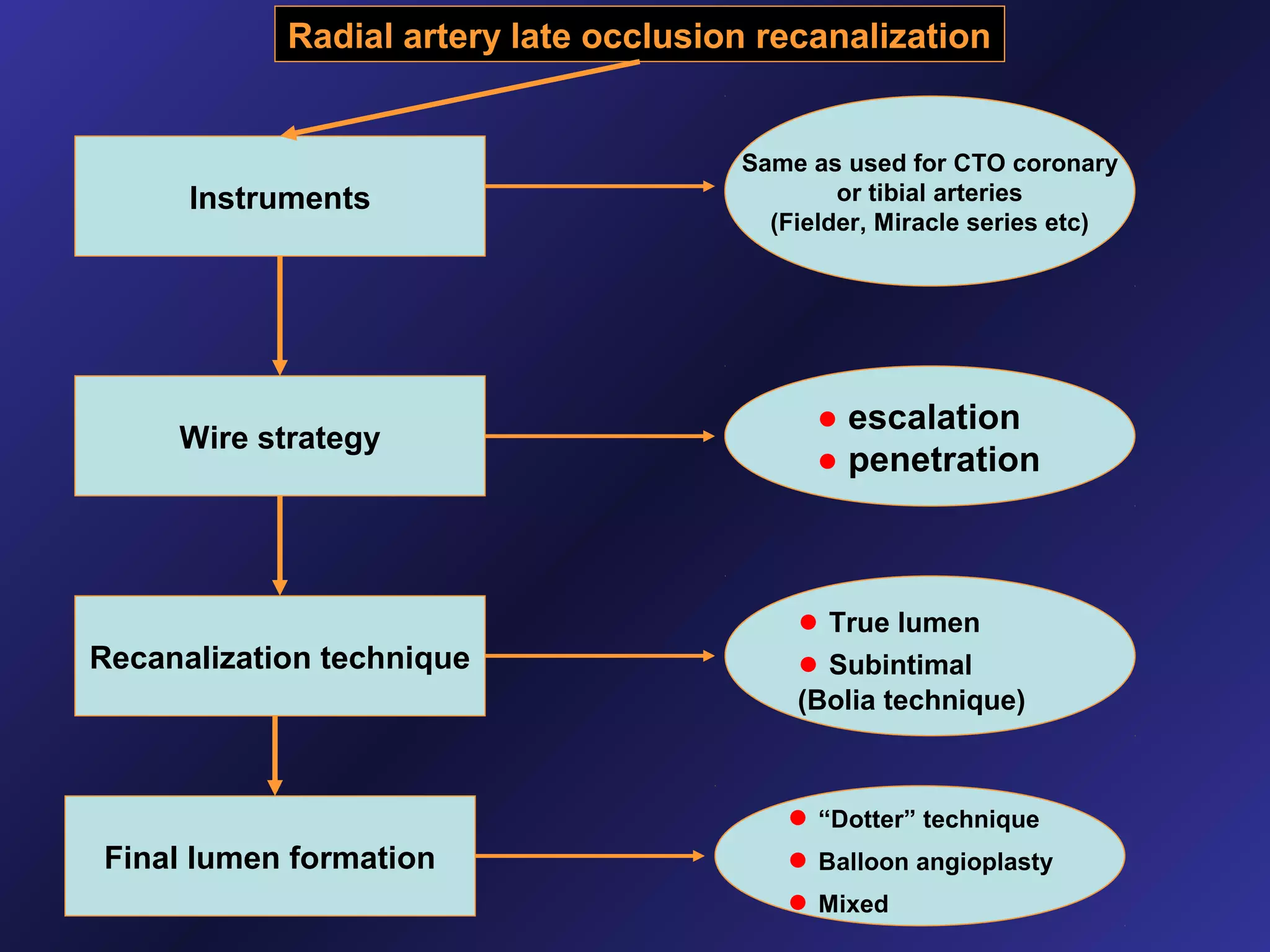
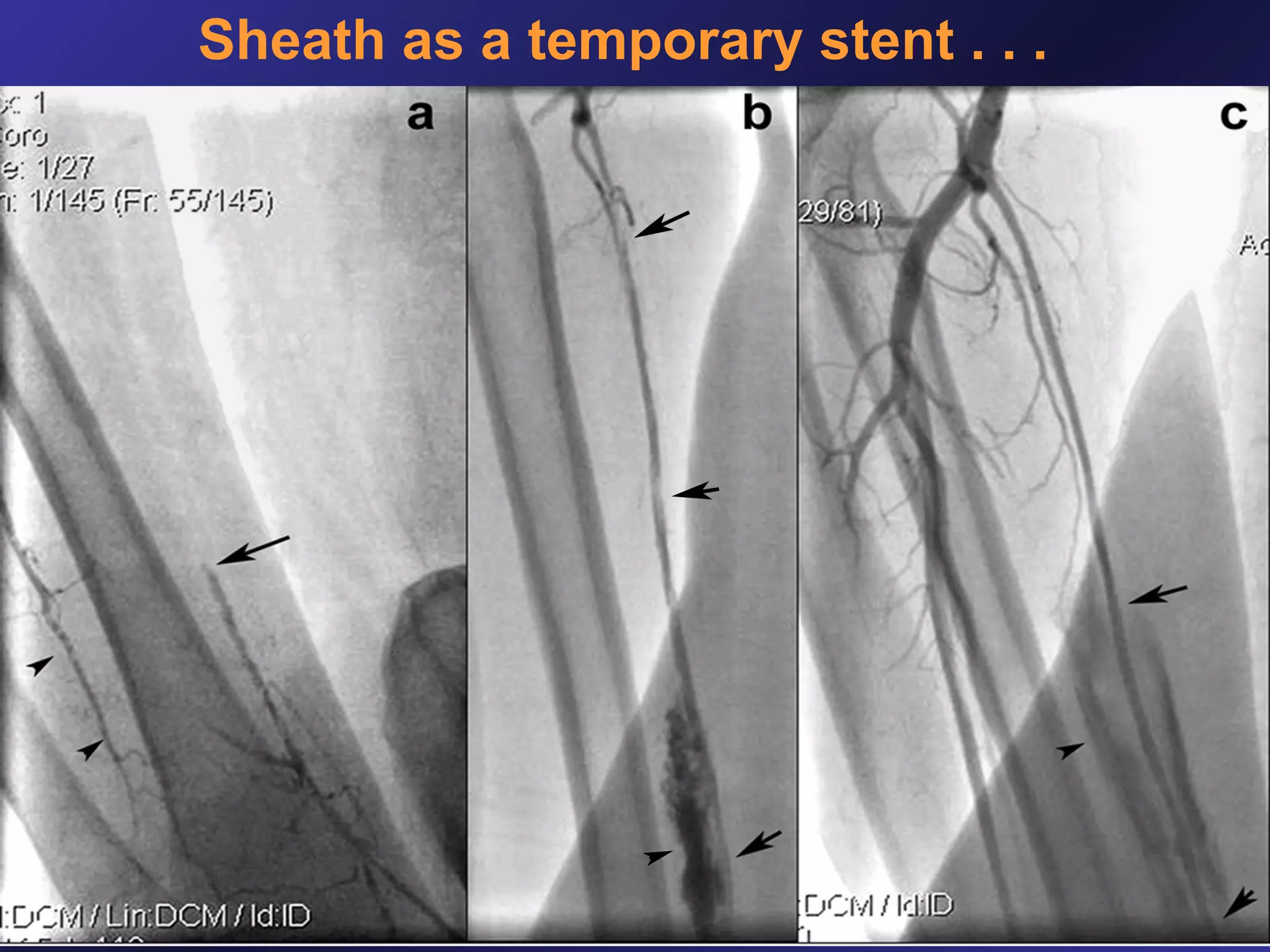
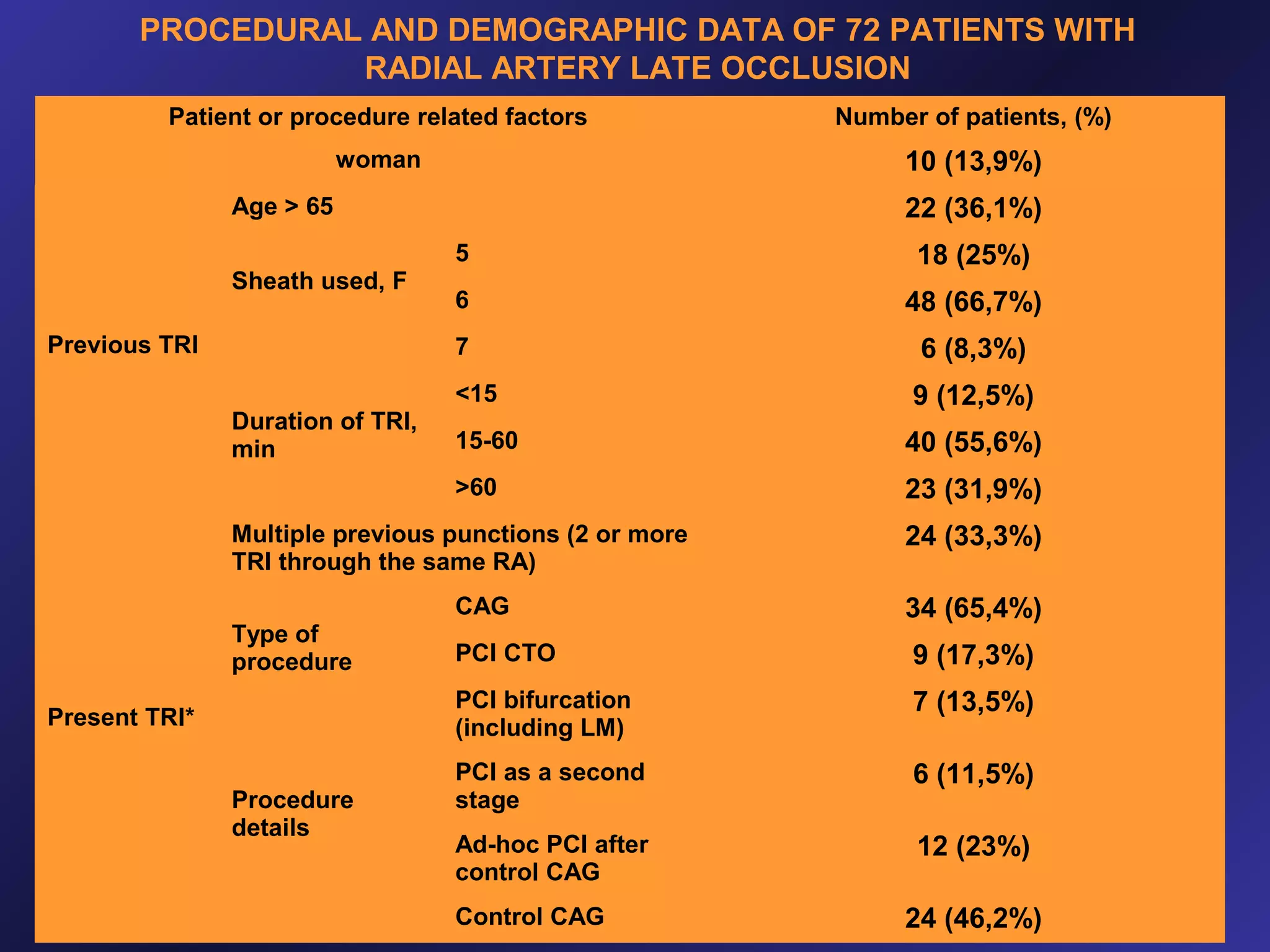
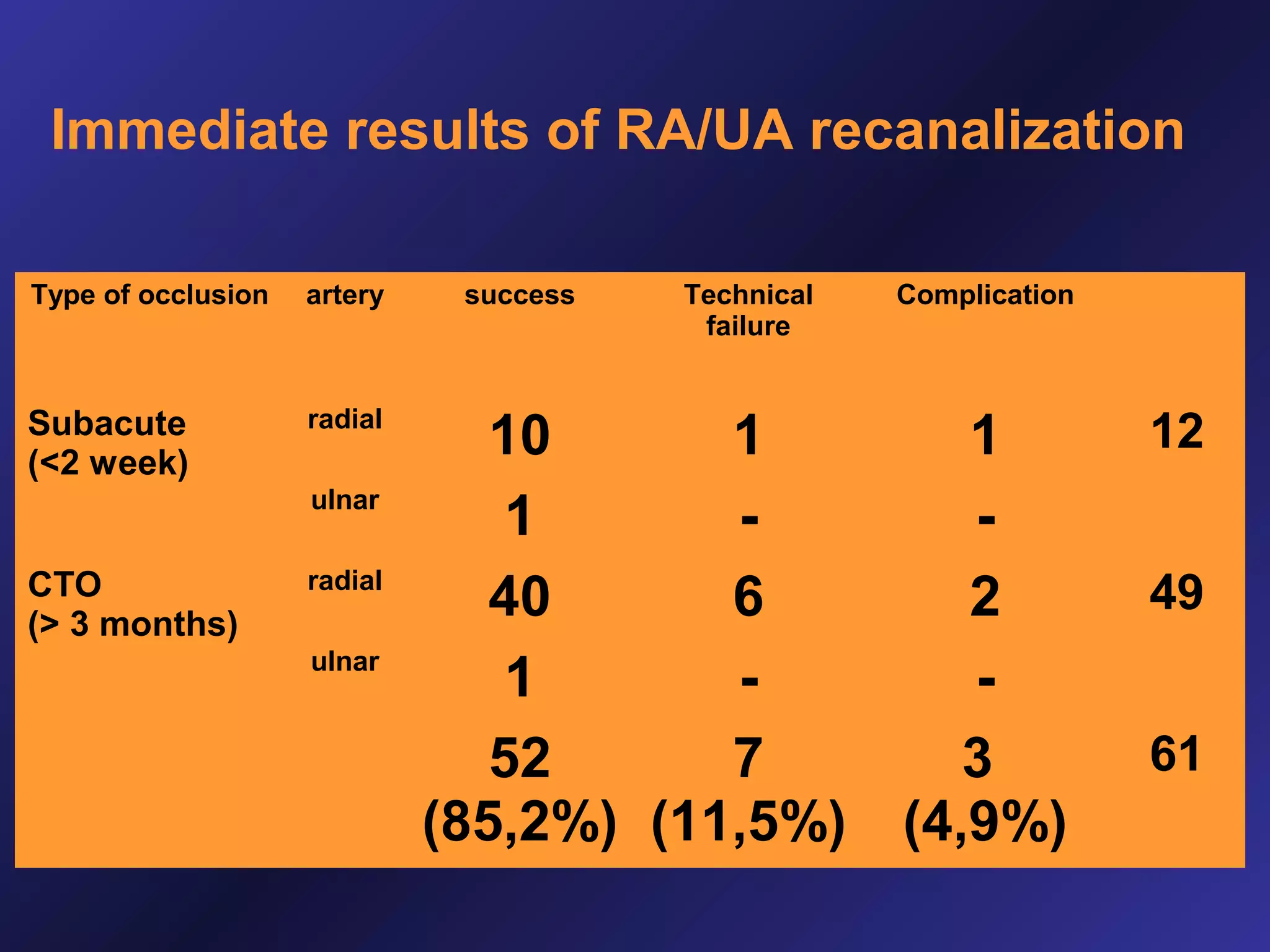
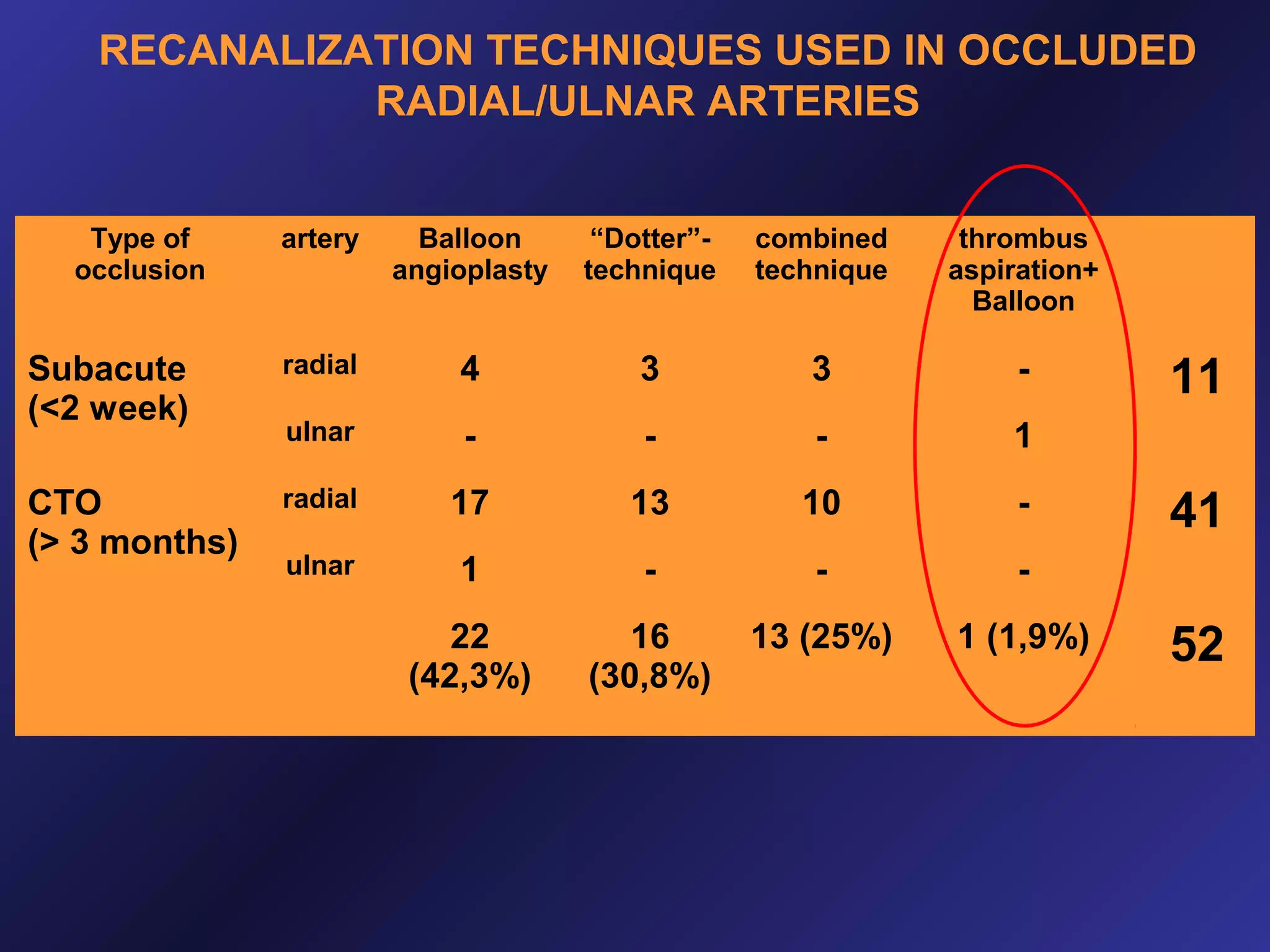
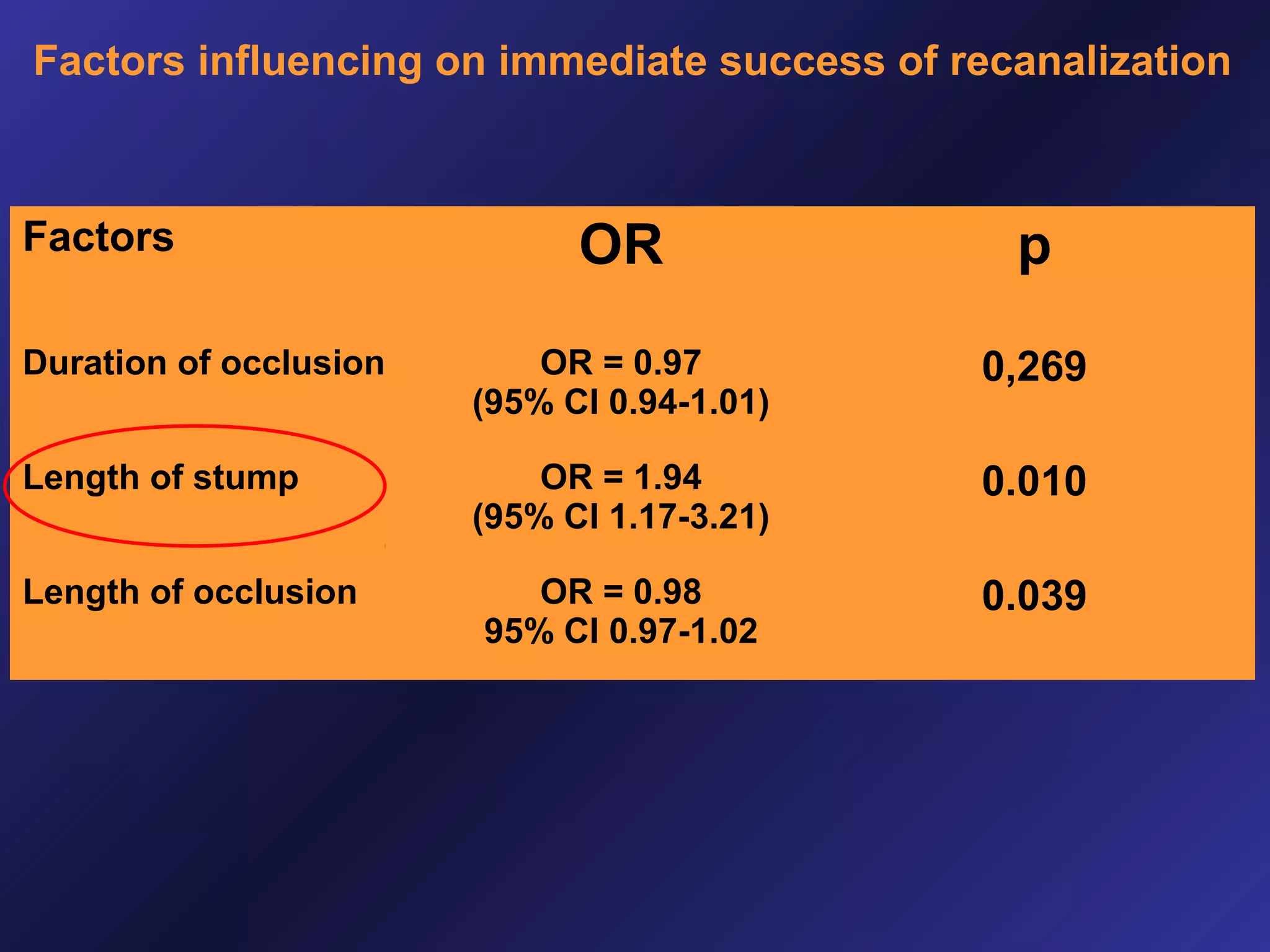
This document discusses the management of late radial artery occlusion during transradial interventions, emphasizing the feasibility and safety of recanalization techniques such as the 'dotter technique' and proximal puncture. A study involving 72 patients revealed that recanalization success rates were acceptable, however, a risk of reocclusion remained. Overall, the document highlights the advantages of these techniques as solutions for challenging arterial access in patients with prior occlusions.























































































