Downloaded 12 times
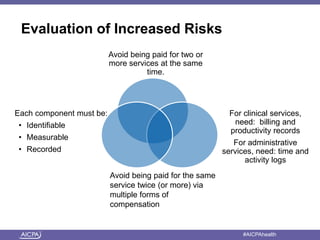
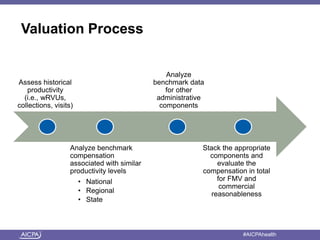
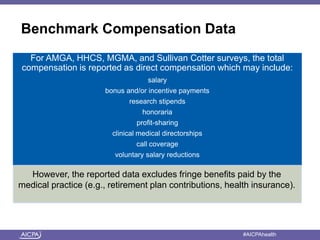
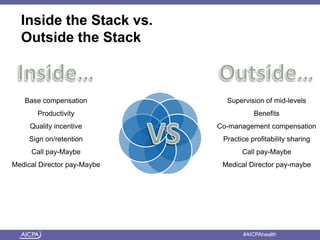
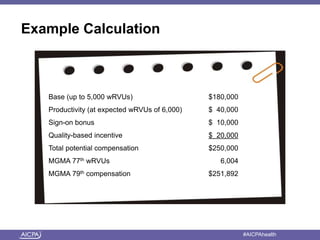
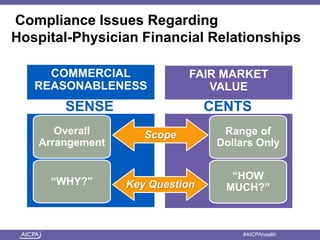


The document summarizes key issues related to physician compensation agreements and the impact of healthcare reform. It discusses the increased complexity of compensation models with multiple layers and components. Ensuring fair market value and commercial reasonableness of the overall arrangement is important as the sum of individual components could exceed what is reasonable. The presentation also covers analyzing losses, benchmarks, and factors considered in commercial reasonableness determinations. Healthcare continues shifting toward value-based payments, quality incentives, and bundled payments through initiatives like Accountable Care Organizations.





















































































