Download as PDF, PPTX


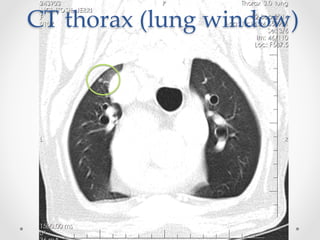
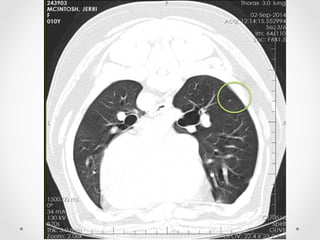
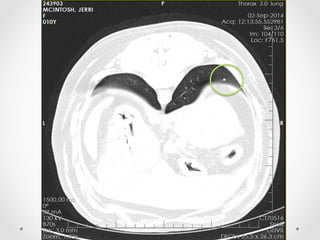
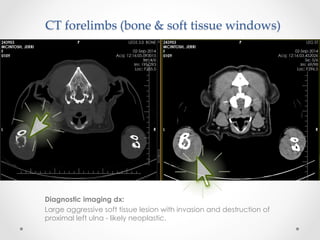
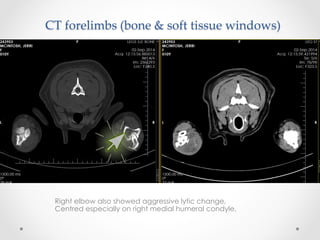
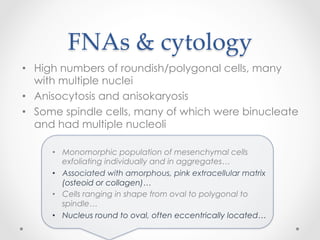




This document discusses the case of a 10-year-old female Rottweiler named Jerri who presented with sudden lameness in her left forelimb. Radiographs and CT scans revealed an aggressive soft tissue lesion invading and destroying the proximal left ulna, likely a neoplasm. Fine needle aspirates of the swelling showed round cells consistent with either osteosarcoma or histiocytic sarcoma. Given the patient's breed and unusual location of the lesion, histiocytic sarcoma could not be ruled out. Treatment options of amputation, radiation therapy, chemotherapy or palliative care were discussed. The owner elected to pursue radiation therapy with the goal of palliation.
![Peripheral blood smear [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/peripheralbloodsmearautosaved-201029200454-thumbnail.jpg?width=640&height=640&fit=bounds)



![Neoplasia [part 1]](https://cdn.slidesharecdn.com/ss_thumbnails/neoplasiapart1-190918152450-thumbnail.jpg?width=640&height=640&fit=bounds)






























