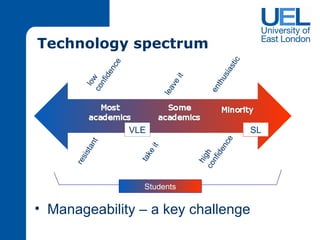
This document summarizes the implementation of a virtual patient system using Second Life at the University of East London. It discusses using Second Life to provide realistic clinical experiences for healthcare students in physiotherapy and herbal medicine programs. The challenges of manageability and sustainability are addressed through a web-based editor to add and modify patient case data and reusable components. Initial feedback from students was positive, but more case development is needed. Expanding the system to other programs like podiatry is also discussed.





![Thanks Contact details [email_address] SL: Justina Dotterkelch [email_address] SL: Maisy Carter](https://image.slidesharecdn.com/hertspresentationjdadditions1006101-100617125245-phpapp01/85/Herts-BLU-Conference-Presentation-170610-23-320.jpg)