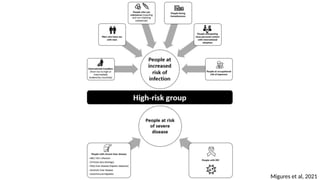
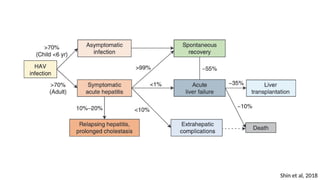
The document provides an overview of hepatitis A and E, detailing their history, epidemiology, transmission, diagnosis, clinical features, treatment, and prevention. Hepatitis A is primarily transmitted via fecal-oral routes and has a significant incidence in developing regions, while hepatitis E transmission typically occurs through contaminated water and can cause severe complications, particularly in pregnant women. Vaccination is key in preventing hepatitis A, with specific guidelines for various risk groups, whereas hepatitis E treatment options are limited and vaccine development is ongoing.

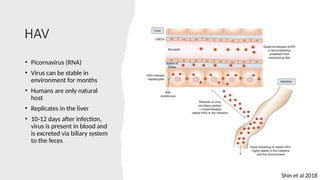













































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















