Acute viral hepatitisis a systemic infection affecting the liver
predominantly.
Almost all cases of acute viral hepatitis are caused by one of
five viral agents: hepatitis A virus (HAV), hepatitis B virus
(HBV), hepatitis C virus (HCV), the HBV-associated delta agent
or hepatitis D virus (HDV), and hepatitis E virus (HEV).
All these human hepatitis viruses are RNA viruses, except for
hepatitis B, which is a DNA virus.
All types of viral hepatitis produce clinically similar illnesses.
3.
These range fromasymptomatic and inapparent to
fulminant and fatal acute infections common to all types,
on the one hand, and from subclinical persistent
infections to
rapidly progressive chronic liver disease with cirrhosis
and even hepatocellular carcinoma.
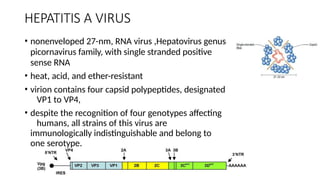
HEPATITIS A VIRUS
•nonenveloped 27-nm, RNA virus ,Hepatovirus genus
picornavirus family, with single stranded positive
sense RNA
• heat, acid, and ether-resistant
• virion contains four capsid polypeptides, designated
VP1 to VP4,
• despite the recognition of four genotypes affecting
humans, all strains of this virus are
immunologically indistinguishable and belong to
one serotype.
6.
• Inactivation ofviral activity can be achieved by
• boiling for 1 minute,
• by contact with formaldehyde and chlorine,
• by ultraviolet irradiation
7.
• Incubation periodof 4 weeks. (15-45 days)
• Replication is limited to the liver
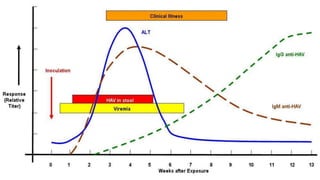
• the virus is present in the liver, bile, stool and blood during the late
incubation period and acute preicteric phase of illness.
• Despite persistence of virus in the liver, viral shedding in feces,
viremia, and infectivity diminish rapidly once jaundice
becomes apparent.
8.
PATHOGENESIS
• After ingestion,the HAV survives gastric acid, moves to the small
intestine and reaches the liver via the portal vein.
• Replicates in hepatocyte cytoplasm
• Not a Cytopathic virus - Immune mediated cell damage more
likely
• Once mature the HAV travels through sinusoids and enters bile
canaliculi, released into the small intestine and systemic circulation,
excreted in feces.
11.
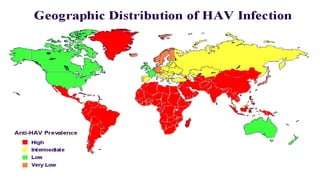
• Has aworldwide distribution.
• The highest seropositivity is observed in adults in urban Africa, Asia,
and South America.
• Acquisition in early childhood is the norm in these nations and
is usually asymptomatic (ANICTERIC HEPATITIS)
• Transmitted almost exclusively by the fecal-oral route
• Factors predisposing humans to early acquisition include
• overcrowding,
• poor sanitation, and
• lack of a reliable clean water resource.
12.
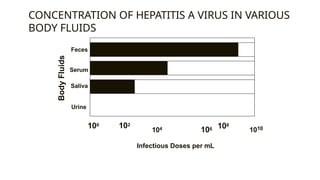
CONCENTRATION OF HEPATITISA VIRUS IN VARIOUS
BODY FLUIDS
Feces
Serum
Saliva
Urine
100 102
104 106
Infectious Doses per mL
108
1010
Body
Fluids
13.
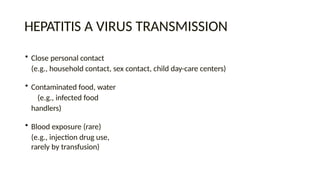
HEPATITIS A VIRUSTRANSMISSION
• Close personal contact
(e.g., household contact, sex contact, child day-care centers)
• Contaminated food, water
(e.g., infected food
handlers)
• Blood exposure (rare)
(e.g., injection drug use,
rarely by transfusion)
14.
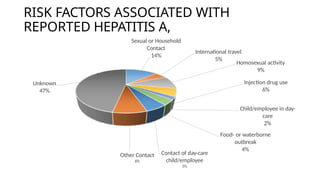
RISK FACTORS ASSOCIATEDWITH
REPORTED HEPATITIS A,
Sexual or Household
Contact
14%
International travel
5%
Homosexual activity
9%
Injection drug use
6%
Child/employee in day-
care
2%
Food- or waterborne
outbreak
4%
Contact of day-care
child/employee
5%
Other Contact
8%
Unknown
47%
15.
PREVENTING HEPATITIS A
•Hygiene (e.g., hand washing)
• Sanitation (e.g., clean water sources)
• Hepatitis A vaccine (pre-exposure)
• Immune globulin (pre- and post-exposure)
16.
PREPARATION OF INACTIVATEDHEPATITIS A
VACCINES
• Cell culture adapted virus grown in human fibroblasts
•Purified product inactivated with formalin
•Adsorbed to aluminum hydroxide adjuvant
17.
• Highly immunogenic
•97%-100% of children, adolescents, and adults have protective levels of antibody
within 1 month of receiving first dose; essentially 100% have protective levels after
second dose
• Highly efficacious
• In published studies, 94%-100% of children protected against clinical hepatitis A
after equivalent of one dose
HEPATITIS A VACCINES
18.
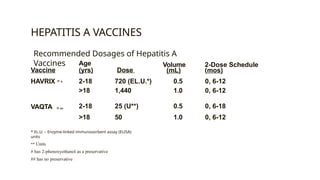
HEPATITIS A VACCINES
Age
(yrs)Dose
Volume
(mL)
2-Dose Schedule
(mos)
Vaccine
HAVRIX ® # 2-18 720 (EL.U.*) 0.5 0, 6-12
>18 1,440 1.0 0, 6-12
2-18 25 (U**) 0.5 0, 6-18
>18 50 1.0 0, 6-12
VAQTA ® ##
* EL.U. – Enzyme-linked immunosorbent assay (ELISA)
units
** Units
# has 2-phenoxyethanol as a preservative
## has no preservative
Recommended Dosages of Hepatitis A
Vaccines
19.
Most common sideeffects
Soreness/tenderness at injection site - 50%
Headache - 15%
Malaise - 7%
No severe adverse reactions attributed to vaccine
Safety in pregnancy not determined – risk likely low
Contraindications - severe adverse reaction to previous dose or allergy
to a vaccine component
No special precautions for immunocompromised persons
SAFETY OF HEPATITIS A VACCINE
20.
DURATION OF PROTECTIONAFTER HEPATITIS A
VACCINATION
• Persistence of antibody
• At least 5-8 years among adults and children
• Efficacy
• No cases in vaccinated children at 5-6 years of follow-up
• Mathematical models of antibody decline suggest protective
antibody levels persist for at least 20 years
• Other mechanisms, such as cellular memory, may contribute
21.
Approved by theFDA in United States for persons >18 years old
Contains 720 EL.U. hepatitis A antigen and
20 μg. HBsAg
Vaccination schedule: 0,1,6 months
Immunogenicity similar to single-antigen
vaccines given separately
Can be used in persons > 18 years old who need vaccination against
both hepatitis A and B
Formulation for children available in many other countries
COMBINED HEPATITIS A HEPATITIS B
VACCINE
22.
• Pre-exposure
• travelersto intermediate and high
HAV-endemic regions
• Post-exposure (within 14 days) Routine household and
other intimate contacts
Selected situations
• institutions (e.g., day-care centers)
• common source exposure (e.g.,
food prepared by infected food handler)
HEPATITIS A PREVENTION IMMUNE GLOBULIN
• Hepatitis Eis an acute disease caused by hepatitis E virus that usually
manifest as acute jaundice.
• Previously labeled epidemic or enterically transmitted non-A, non-B
hepatitis
• Is an enterically transmitted self-limited infection.
• Hallmarks of the disease are high attack-rate in young adults and high
mortality in pregnant women
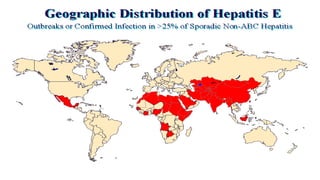
• Spread by fecally contaminated water within endemic areas
• Outbreaks can be epidemic and individual.
25.
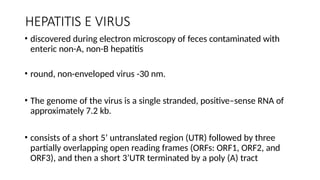
HEPATITIS E VIRUS
•discovered during electron microscopy of feces contaminated with
enteric non-A, non-B hepatitis
• round, non-enveloped virus -30 nm.
• The genome of the virus is a single stranded, positive–sense RNA of
approximately 7.2 kb.
• consists of a short 5’ untranslated region (UTR) followed by three
partially overlapping open reading frames (ORFs: ORF1, ORF2, and
ORF3), and then a short 3’UTR terminated by a poly (A) tract
26.
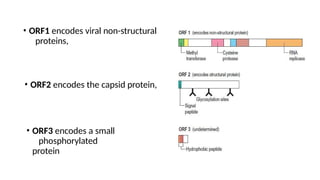
• ORF1 encodesviral non-structural
proteins,
• ORF2 encodes the capsid protein,
• ORF3 encodes a small
phosphorylated
protein
27.
• Classified tentativelyinto four major genetic groups (genotype 1-4)
• Genotype 1 is further segregated into five subgroups, subtypes 1a to
1e.
• Genotype 1c was observed only during 1996 to 1998
MORTALITY/MORBIDITY:
• The overallcase fatality rate is 4%.
• The case fatality rate among pregnant women is 20%, which increases
during the second and third trimesters.
• Reported causes of death include encephalopathy and disseminated
intravascular coagulation.
• The rate of fulminant hepatic failure in infected pregnant women is high.
• Predominantly affects those aged 15-40 years.
• May affect younger age groups but generally is not recognized and may
be subclinical.
• No chronic cases have been described.
HEPATITIS E INPREGNANCY
• High incidence of death from acute hepatic failure in pregnant women is
recognized as a distinct characteristic feature of hepatitis E.
• Pregnant women are not found to be more prone to HE, but the
incidence of AHF is higher among pregnant women during the
epidemics
• It was more common in 3rd trimester (41%), compared to 1st trimester
(20%) or 2nd trimester (26%).
• Majority of patients with AHF are young (78% were aged below 25
years age) and primi-gravida (70%)
33.
• No immunoprophylaxisis available.
• Immunoglobulin from infected patients is not effective in preventing
outbreaks or sporadic cases.
• Prototype vaccines are being developed using animal models.
• this is hindered by an inability to maintain the virus in cell cultures.
• Once infection occurs, therapy is limited to support.
• Provide patients with adequate hydration and electrolyte repletion.
PREVENTION




































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











