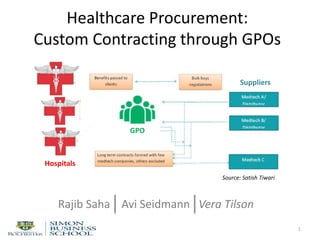

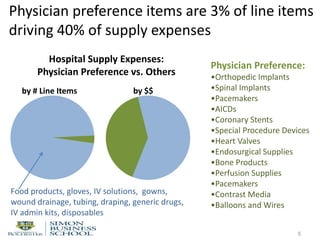
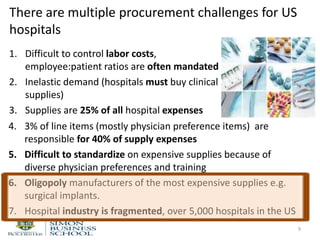
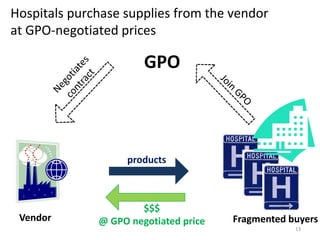


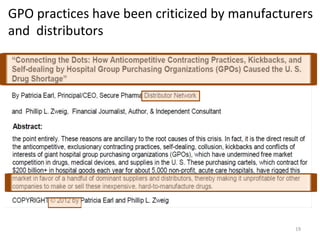
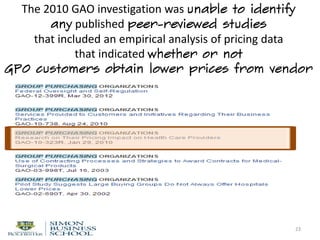
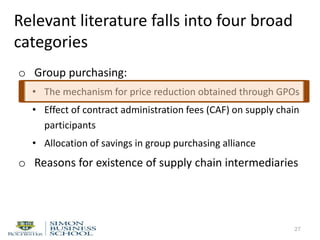
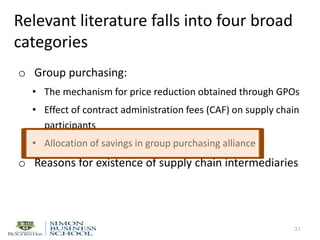
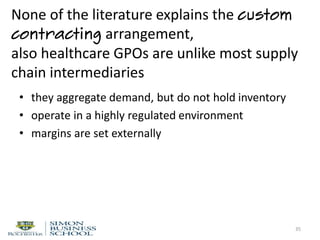

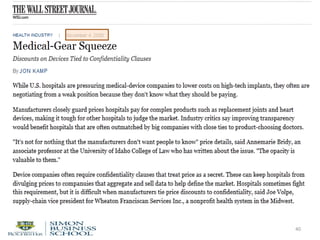
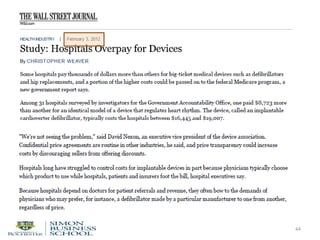

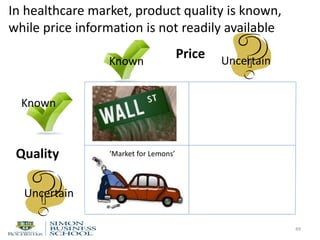

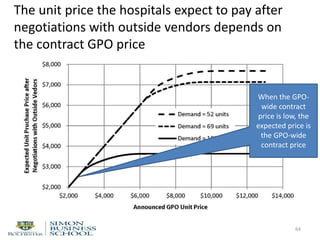
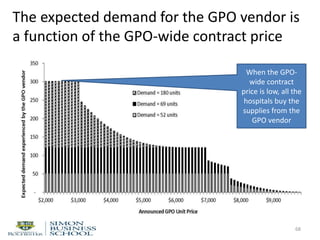
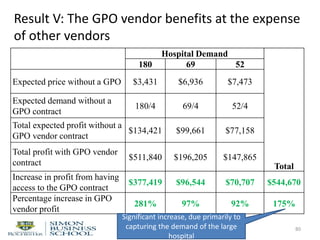
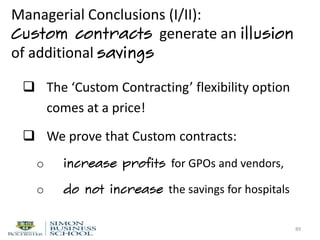
![Assumption III: Price attainable through vendor-
hospital negotiations is random &
stochastically decreasing in demand
51
Upper limit on attainable
price
Lower limit on
attainable price
PurchasePrice,$/unit
Expected price
Hospitals’ purchase volume [units/period]](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-51-320.jpg)
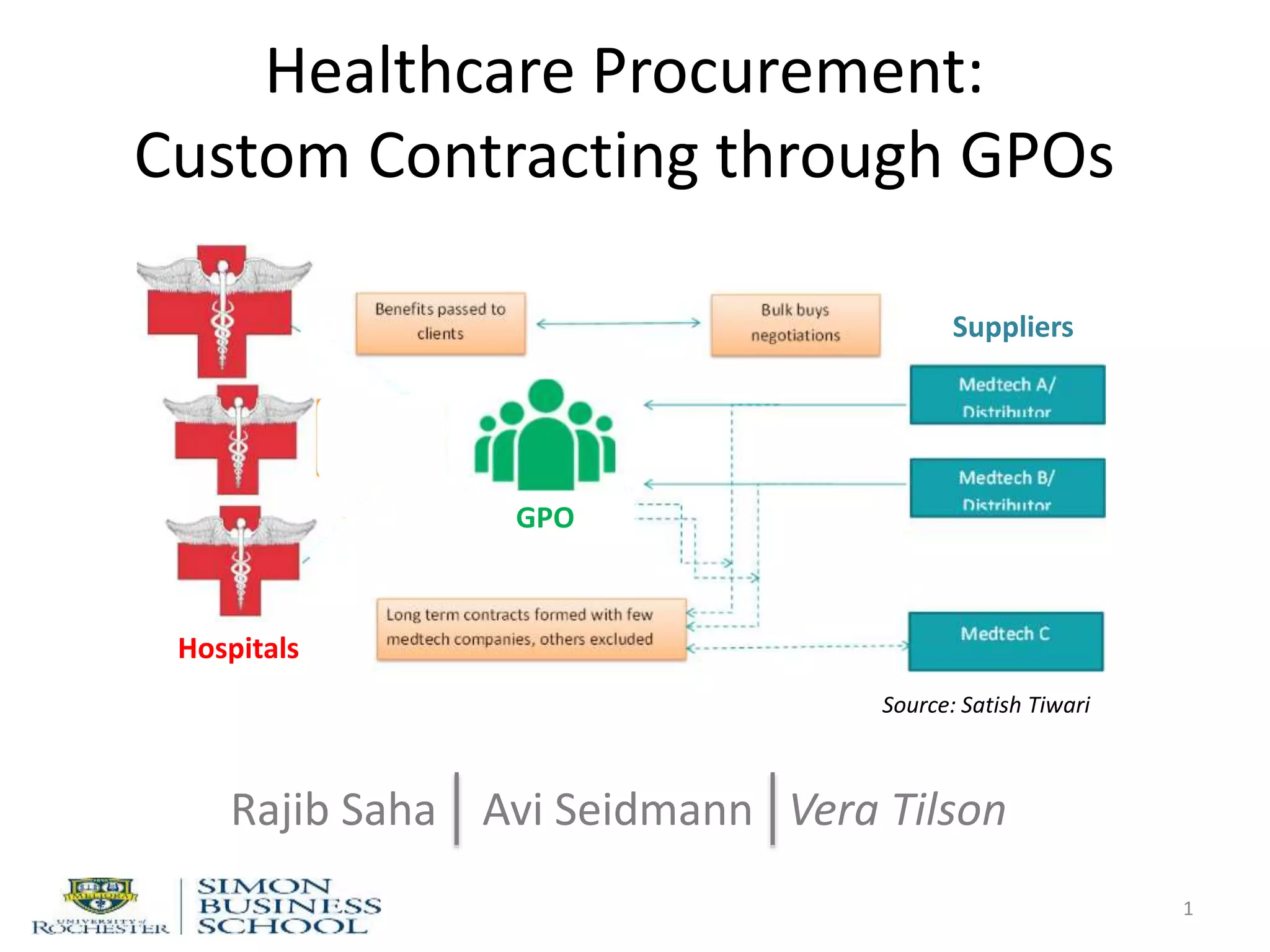
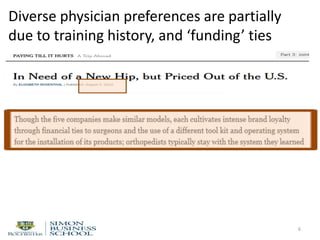
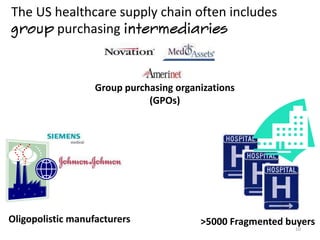
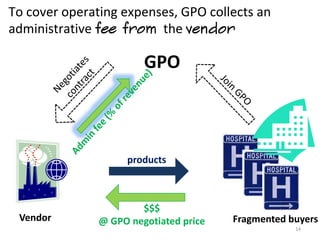
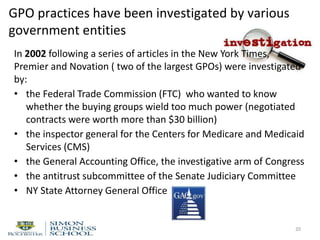
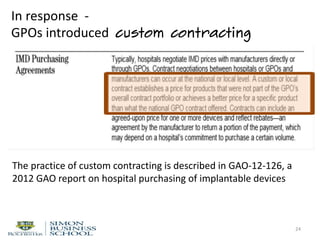
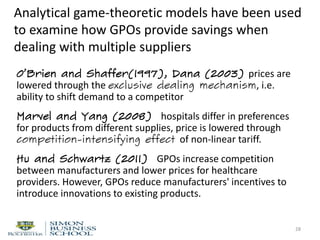
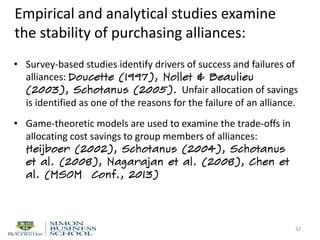
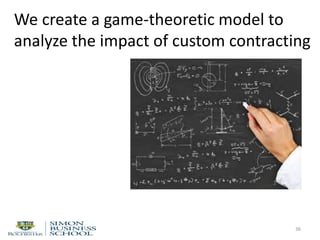
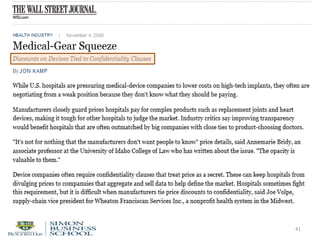
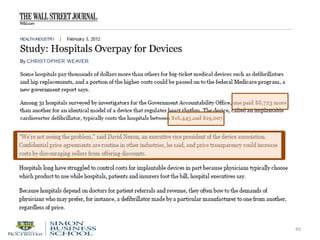
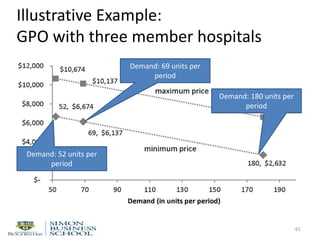
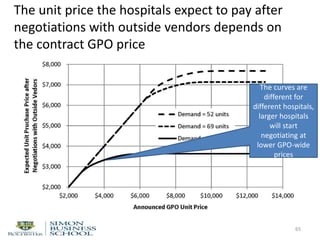
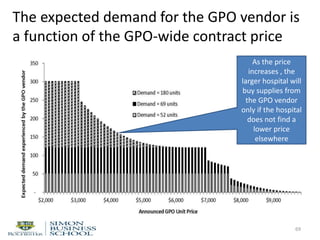
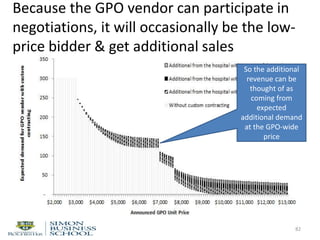
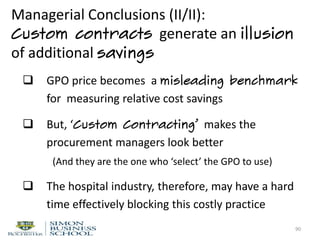
![Assumption IV: GPO member hospitals are
heterogeneous in terms of demand volume.
This distribution is known to the GPO vendor.
52
#ofmemberhospitals
Hospitals’ purchase volumes [units/period]](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-52-320.jpg)
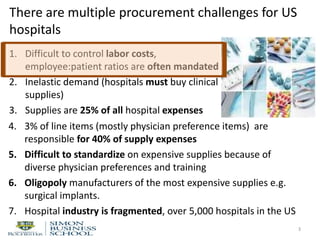
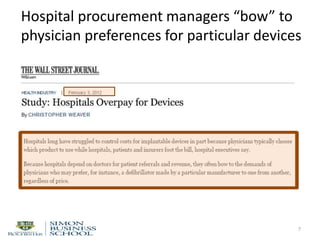
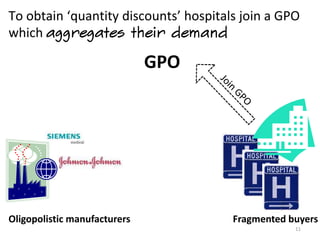
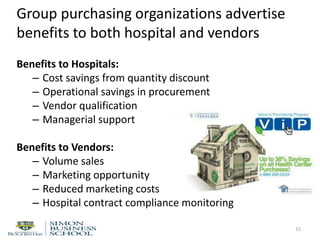
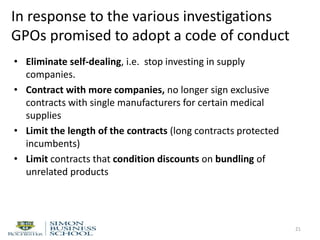
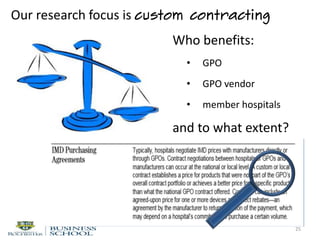
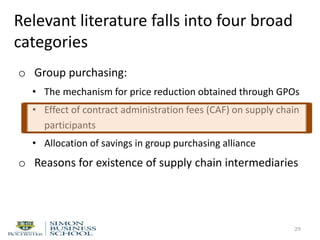
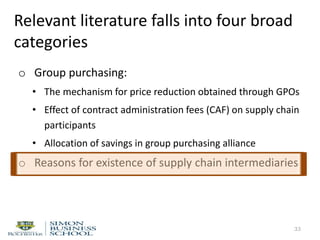
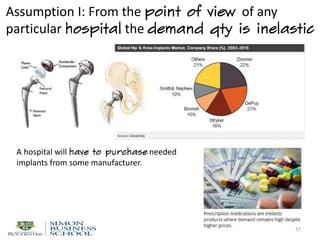
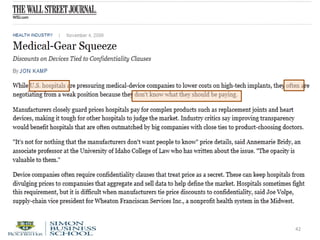
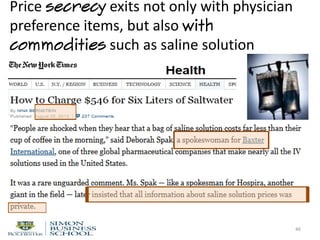
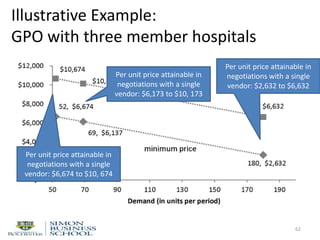
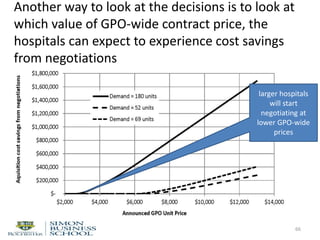
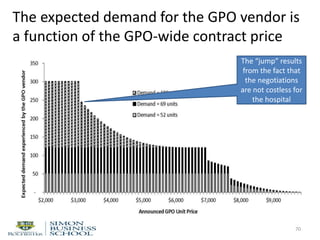
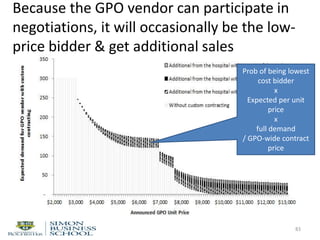
![Assumption V: Decision timing
53
TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
GPO-selected vendor sets the
GPO-wide contract price for all
members](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-53-320.jpg)
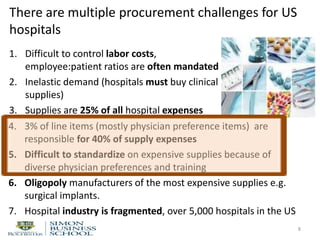
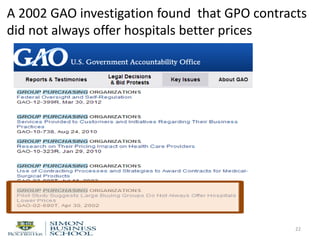
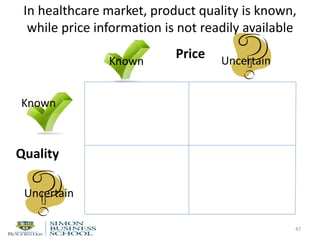
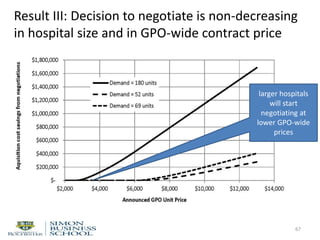
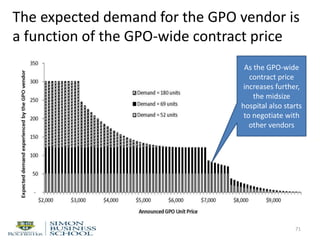
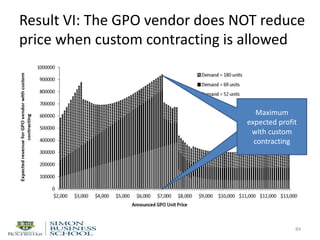
![Assumption V: Decision timing
54
TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
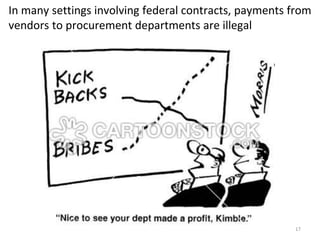
Hospital decides whether to
purchase supplies at this price,
or to negotiate with other
vendors](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-54-320.jpg)
![Assumption V: Decision timing
55
TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
If the hospital is able to find a
lower price from another vendor,
it purchases supplies from that
vendor. Otherwise, from the GPO
vendor at the general price](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-55-320.jpg)
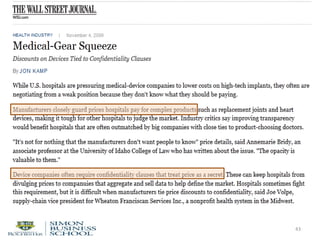
![Assumption V: Decision timing
56
TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
When custom contracting is
allowed, a hospital can invite
the GPO vendor to
participate in custom
negotiations](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-56-320.jpg)
![Assumption V: Decision timing
57
TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
The GPO vendor can choose
to participate or not to
participate](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-57-320.jpg)
![Assumption V: Decision timing
58
TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
The hospital will purchase
supplies at the lowest
negotiated price](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-58-320.jpg)
![TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
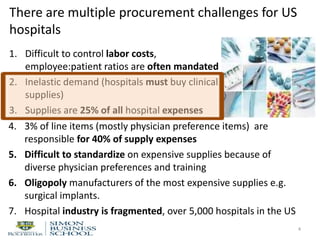
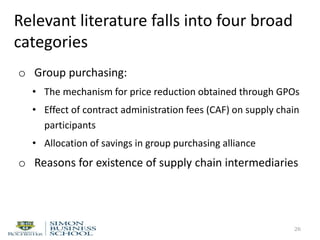
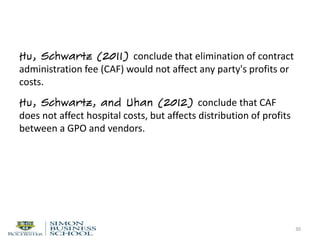
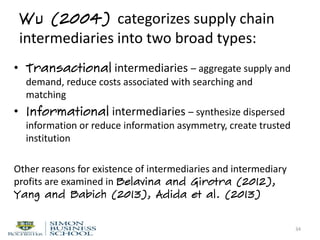
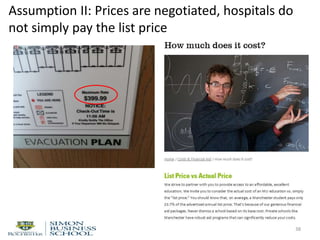
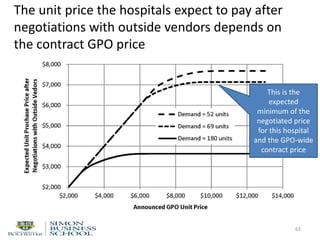
Result I: The GPO vendor is never worse off
with custom contracting
59
The GPO vendor can always
refuse to participate in
custom negotiations](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-59-320.jpg)
![TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
Result II: The GPO is never worse off with
custom contracting
60
If the GPO vendor agreed to
participate means that its
expected revenue is higher
than when it does not
participate](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-60-320.jpg)
![TreePlan Trial Version, For Evaluation Only www.TreePlan.com
Hospital: don't negotiate
0
0 0
0.5
Negotiated price above GPO price
0
0 0
1
0 0 0 0.5
Negotiated price below GPO price
0
0 0
Hospital: negotiate 0.5
1 Negotiated price above GPO price
0 0 0
0 0
0 0 0.5
Negotiated price below GPO price
0
0 0
1
0 0 0.5
Negotiated price above GPO price
0
0 0
GPO vendor: participate
0.5
0 0 GPO vendor selected
0.5 0
0 0
0 0 0.5
GPO vendor not selected
0
0 0For Evaluation Only
GPO
vendor
set price
Pg
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
q P g - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
Hospital:invite GPO
vendor
Hospital: don't
invite GPO vendor
GPO vendor: don't
participate
Negotiated price
below GPO price
λ q P g q P g + c (k,0 )
0 q E [p (q,P g ,0 ) | p <P g ] + c (k,0 )
λ q E [p (q,P g ,1 ) | p <P g ] - k v q E [p (q,P g ,1 ) | p <P g ] + c (k,1 )
GPO vendor payoff Hospital cost
λ q P g q P g
λ q P g - k v q P g + c (k,1 )
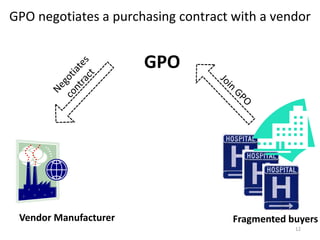
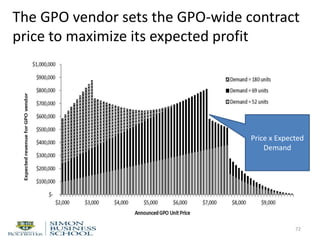
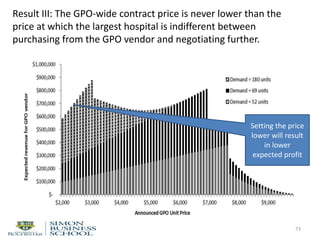
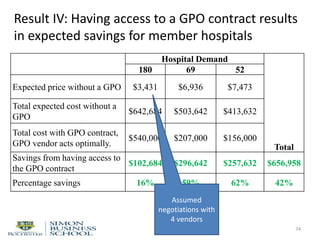
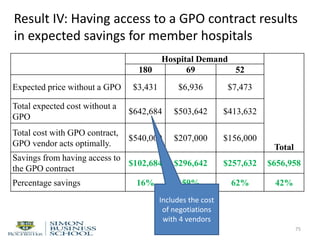
Next, we take a closer look at custom contracting
81](https://image.slidesharecdn.com/gpopresentation151019olin-151218175544/85/Healthcare-Procurement-Custom-Contracting-through-GPOs-81-320.jpg)
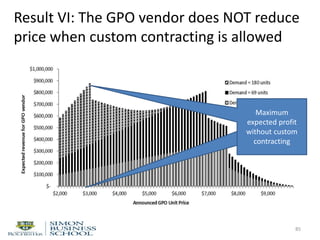


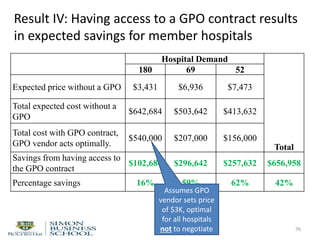
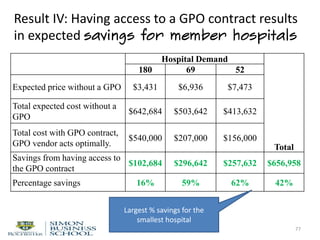
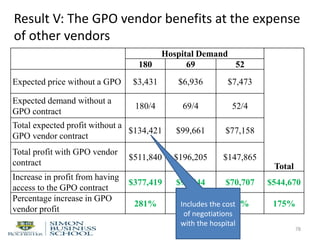
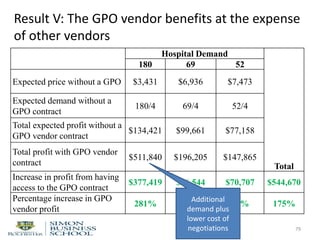
The document discusses procurement challenges faced by US hospitals, highlighting issues such as high labor costs, inelastic demand for clinical supplies, and the significant financial impact of physician preference items. It also outlines the role of group purchasing organizations (GPOs) in mitigating some of these challenges by negotiating better prices through aggregated demand, although GPO practices have faced scrutiny and calls for reform. The analysis includes exploration of custom contracting arrangements and their implications on cost-efficiency and relationships among hospitals, vendors, and GPOs.





















































































