Downloaded 26 times

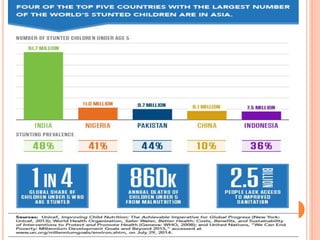


This document summarizes the key topics of health, sanitation, and related issues in India. It discusses definitions of health and its determinants. Major health issues in India include high rates of child malnutrition, infant mortality, diseases, and lack of access to safe drinking water and proper sanitation. Poor sanitation contributes to the spread of infectious diseases and is a potential cause of malnutrition. Rural health care services remain inadequate. The document outlines various approaches to improving sanitation and waste management in India.



































![Enciclopedia einaudi [1982] - elenco Pacchetti_Lemmi](https://cdn.slidesharecdn.com/ss_thumbnails/enciclopediaeinaudi1982-elencopacchettilemmi-141231112253-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)













































