Downloaded 214 times



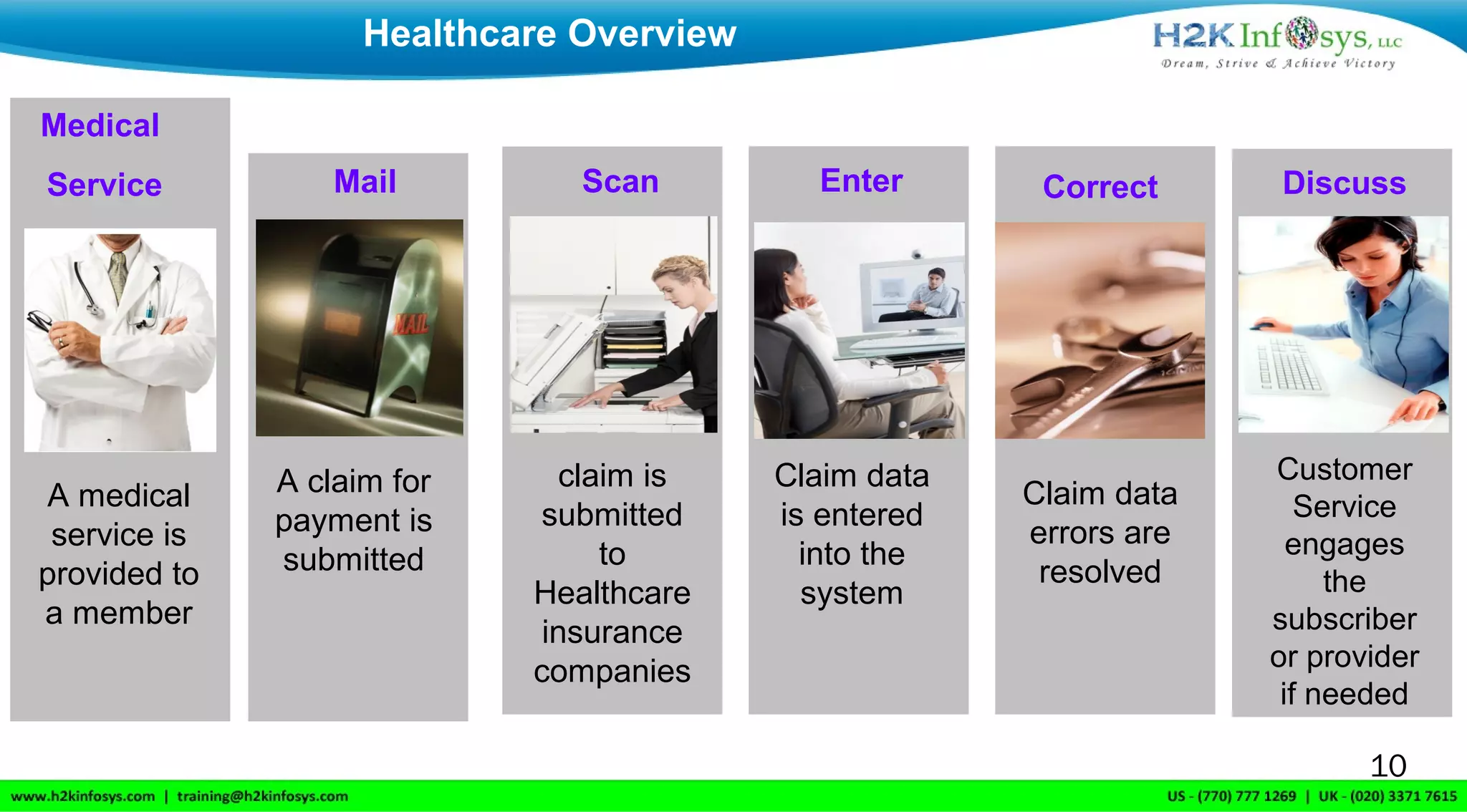
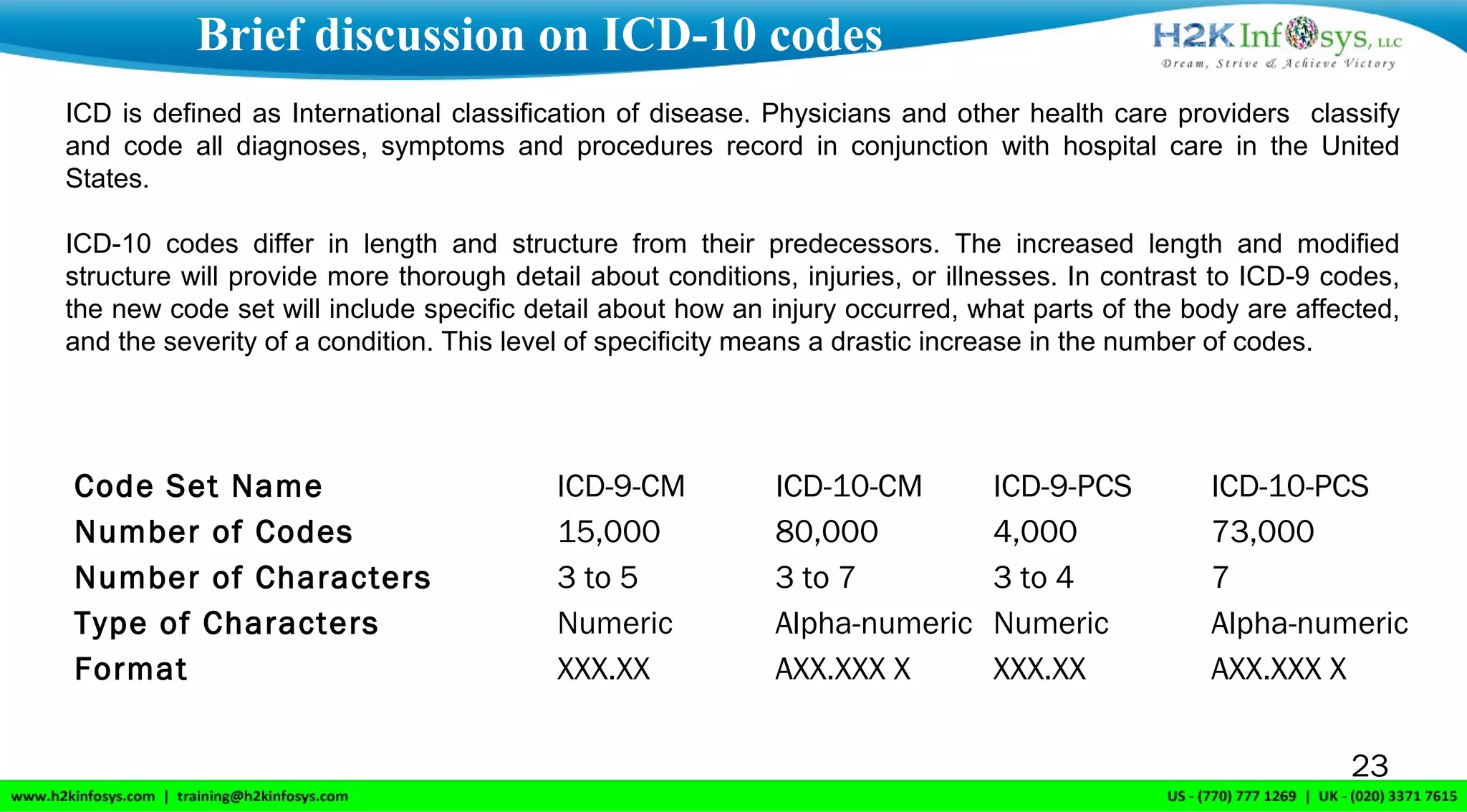

H2K Infosys, based in Atlanta, Georgia, offers online IT training services globally, focusing on healthcare and insurance processes. The document outlines key terminologies such as claims, benefits, and the roles of members and providers within the healthcare system, as well as the lifecycle of a claim from submission to payment. It also discusses the transition from ICD-9 to ICD-10 coding, emphasizing the improved specificity and details in the new coding system.

































































































