Download to read offline

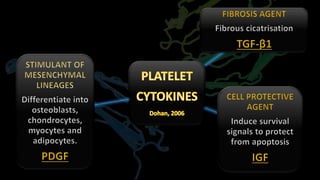

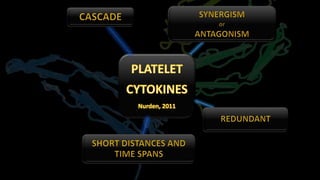
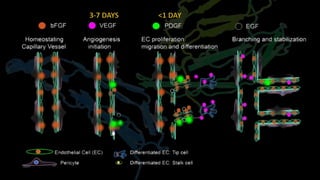
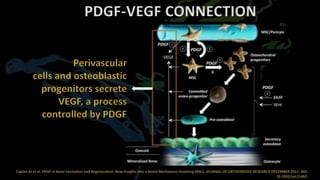

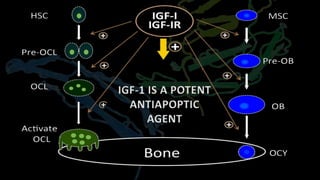
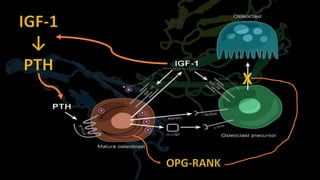
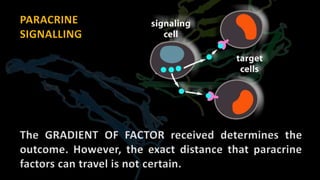
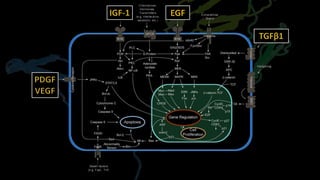


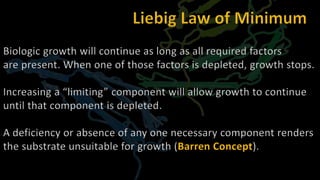
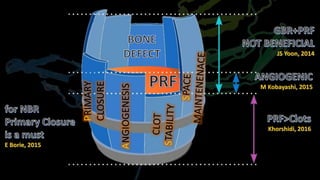
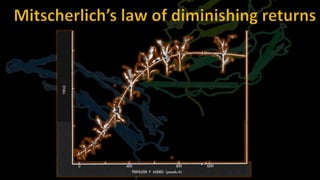
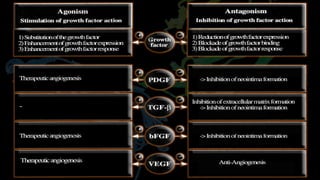

The document discusses the applications and limitations of platelet cytokines in dental procedures, particularly focusing on their role in bone regeneration and stability. It highlights significant findings regarding the efficacy of growth factors, such as IGF-1, and emphasizes that growth processes are contingent upon the availability of all necessary components. Moreover, it outlines the implications of factor depletion on biological growth and angiogenesis.







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














