Downloaded 47 times
![MITIGATION STRATEGY
Promote personal hygiene, environmental sanitation,
safe drinking water and food safety (with leadership
from Ministry of Rural Development).
Integrate household food and nutrition security
considerations into the design of cropping and
farming systems (with leadership from the Ministry of
Agriculture).
Expand and improve nutrition education and
awareness as well as involvement and accountability
for improved nutrition at the community level (with
leadership from the Ministry of Women and Child
Development and the Ministry of Panchayati Raj
[local self government] and including others, such as
the Ministry of Information and Broadcasting and the
Department of Education).](https://image.slidesharecdn.com/goldenjubleeseminar-130813071746-phpapp02/85/NUTRITIONAL-ANTHROPOLOGY-Learning-for-Success-JHARKHAND-12-320.jpg)
![CONVERGENCE (POSSIBILITIES WITH OTHER /RELATED EFFORTS)
Based on the Indian context and significant
programming experience, following are the ways to
improve nutrition.
Expand efforts to engage and empower vulnerable
communities, particularly women in these
communities, to overcome malnutrition (including
through Gram Sabhas [local councils] and self help
groups).
Ensure that nutrition related programmes focus on
key nutrition outcomes and are reaching the priority
target groups of children under two years of age, and
women (especially adolescent girls, pregnant women
and lactating mothers) in order to break the
intergenerational cycle of malnutrition and to achieve
the desired result](https://image.slidesharecdn.com/goldenjubleeseminar-130813071746-phpapp02/85/NUTRITIONAL-ANTHROPOLOGY-Learning-for-Success-JHARKHAND-13-320.jpg)


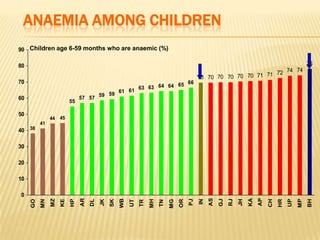
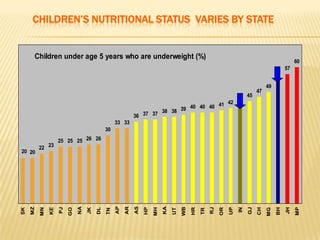
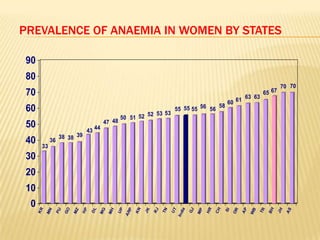
This document discusses malnutrition in the state of Jharkhand, India. It finds that: - Anaemia and underweight rates among children and women in Jharkhand are among the highest in India. - Government runs supplementation programs for iron, folic acid, and Vitamin A, but coverage is low. - It recommends focusing on proven interventions like breastfeeding, complementary feeding, and nutrition for women and children to reduce malnutrition. - A multisectoral approach is needed across health, agriculture, education and other areas to effectively address the problem.



















































































