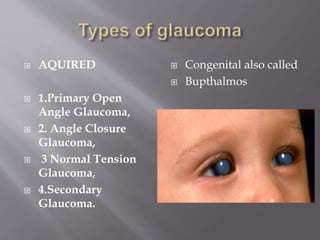
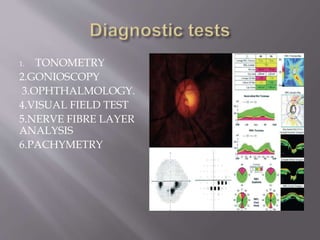
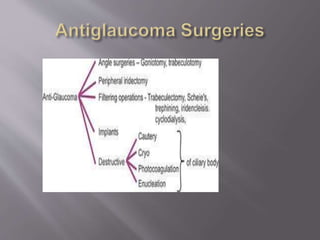
Glaucoma is a group of eye diseases that can cause vision loss and blindness by damaging the optic nerve. There are different types of glaucoma including open-angle glaucoma, which is chronic, progressive, and irreversible. Glaucoma affects over 70 million people worldwide and is the second leading cause of blindness. Risk factors for glaucoma include older age, family history, elevated intraocular pressure, and certain medical conditions. Glaucoma is diagnosed through tests such as tonometry, gonioscopy, visual field tests, and analysis of the nerve fiber layer and treated through prescription eye drops, laser therapy, or surgery.