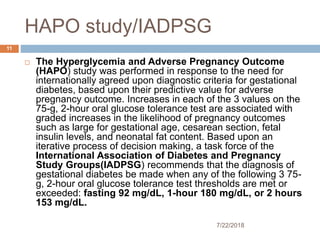
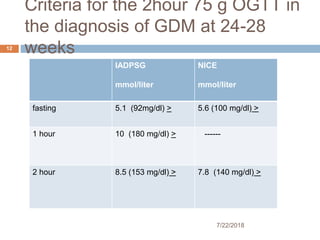
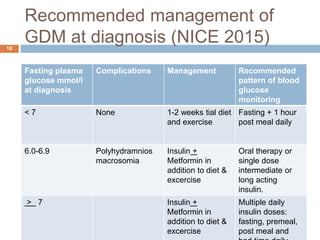
Gestational diabetes mellitus (GDM) is a type of diabetes that is first recognized during pregnancy. An oral glucose tolerance test is used to diagnose GDM, with abnormal fasting or post-meal blood glucose levels indicating GDM. Women with GDM are at higher risk of complications during pregnancy like preeclampsia and delivering a large baby, so treatment focuses on maintaining normal blood glucose levels through diet, exercise, and possibly insulin or metformin. After delivery, women with GDM have an increased long-term risk of type 2 diabetes and should undergo screening.