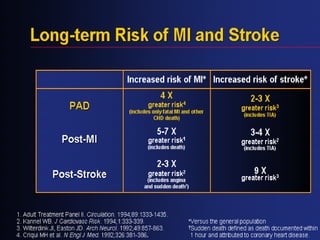
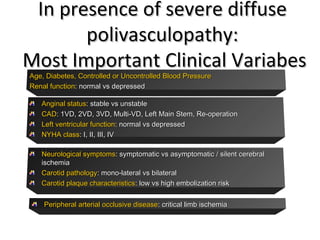
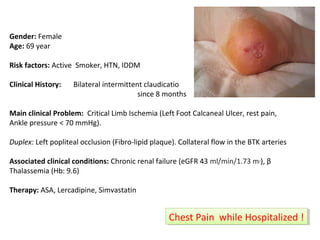
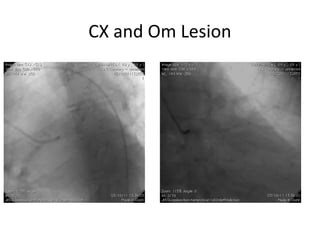
1) This document discusses a case of a female patient presenting with critical limb ischemia and diffuse polyvascular disease including coronary artery disease.
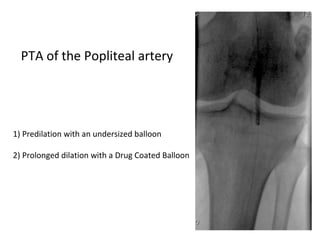
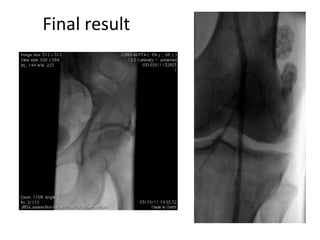
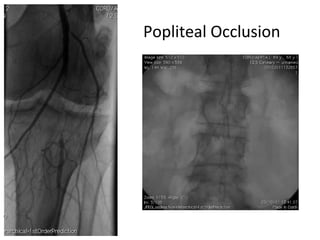
2) Treatment involved percutaneous angioplasty of the occluded left popliteal artery using a drug-coated balloon, with optimization of medical therapy for her coronary artery disease.
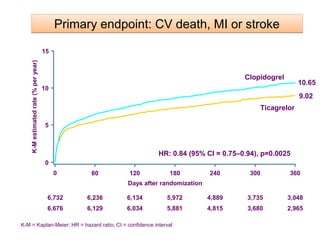
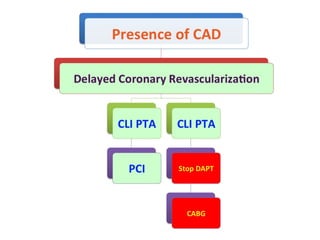
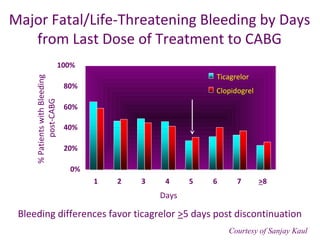
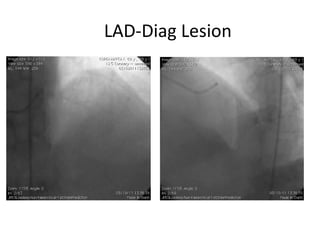
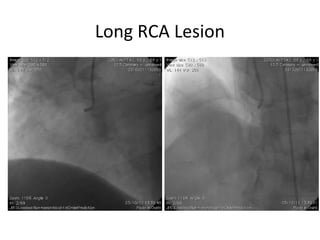
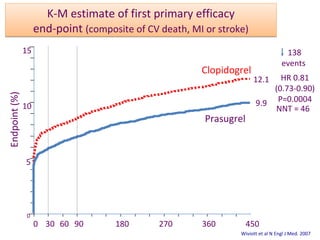
3) The document emphasizes the importance of evaluating and managing concomitant coronary artery disease in patients with peripheral artery disease to achieve good long-term outcomes, and discusses optimal antiplatelet therapy choices to balance ischemic and bleeding risks.

![2.5
2
1.5
1
0.5
0
DDeeffiinniittee//PPrroobbaabbllee SSTT:: AAnnyy SStteenntt ((NN==1122884444))
52%
STENT Analysis
0 50 100 150 200 250 300 350 400 450
% of Subjects
HR 0.48 [0.36-0.64]
P<0.0001
1 year: 1.06 vs 2.15%
HR 0.48 [0.36-0.65], P<0.0001
2.35%
1.13%
DAYS
CLOPIDOGREL
PRASUGREL
Wiviott SD et al. Lancet 2008
Definite/Probable But remember limitations!!!!](https://image.slidesharecdn.com/generalisedatherosclerosis-drantoniomicari-141023142242-conversion-gate02/85/Generalised-atherosclerosis-dr-Antonio-Micari-16-320.jpg)