Download to read offline

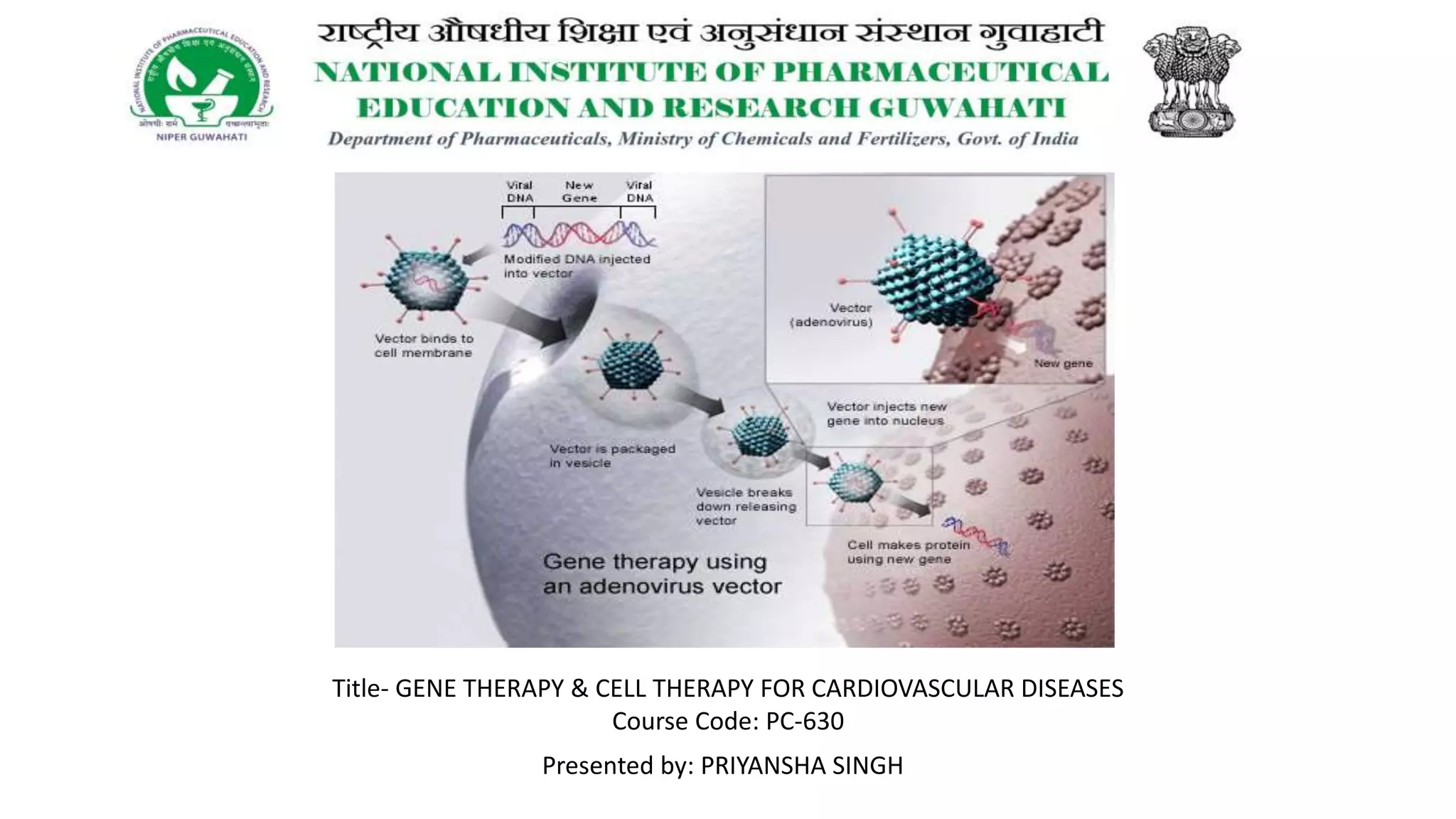
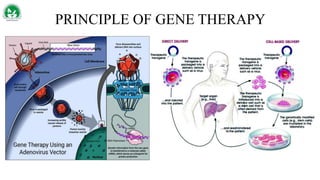

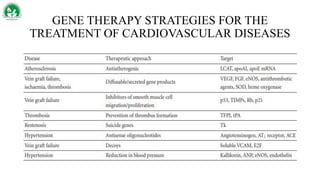
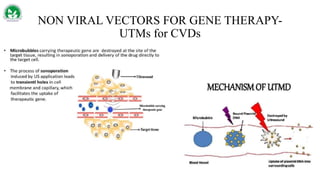

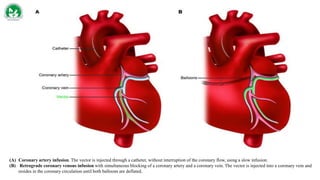
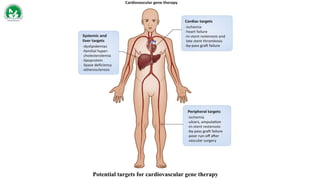
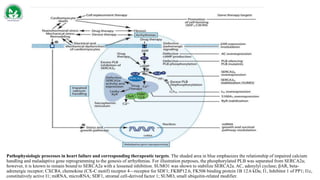
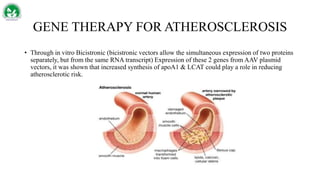
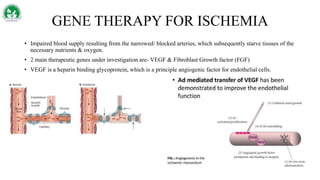
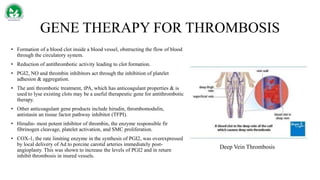
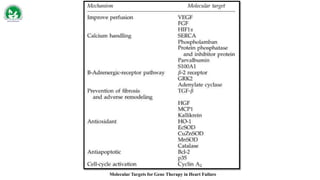
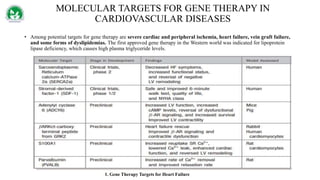
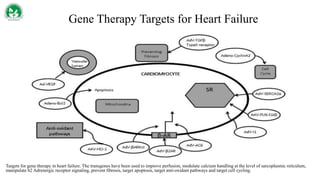
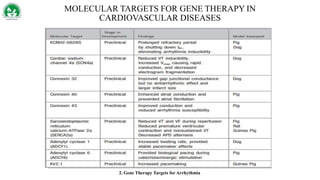
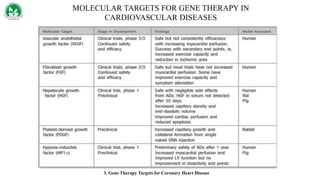

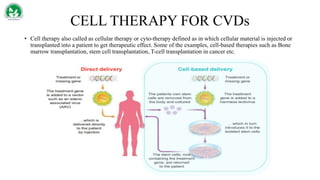
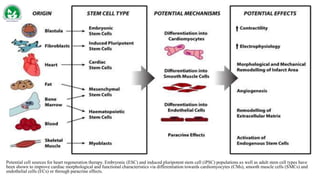


Gene therapy and cell therapy hold promise for treating cardiovascular diseases. The document discusses gene therapy strategies using viral and non-viral vectors to target conditions like heart failure, atherosclerosis, and ischemia. Key molecular targets discussed for heart failure include SERCA2a, SDF-1, and genes involved in calcium handling. Challenges for cardiovascular gene therapy include developing efficient methods for delivering gene vectors to target tissues.













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









