Download to read offline
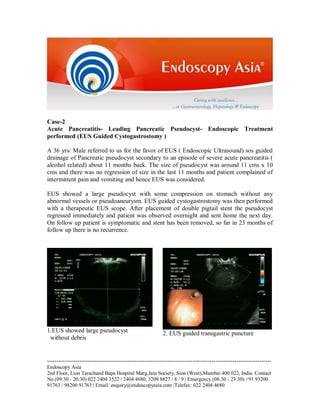





A 36-year-old male with a pancreatic pseudocyst resulting from severe acute pancreatitis underwent endoscopic ultrasound-guided cystogastrostomy, leading to immediate regression of the cyst and no recurrence after 23 months. Another case involved a 48-year-old female with rectal bleeding, diagnosed with a polyp at the recto-sigmoid junction, who successfully had the polyp removed via endoscopic polypectomy. Both cases underscore the efficacy of endoscopic techniques in managing symptomatic gastrointestinal conditions.



































































