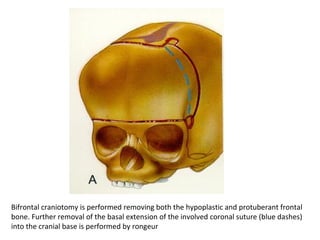
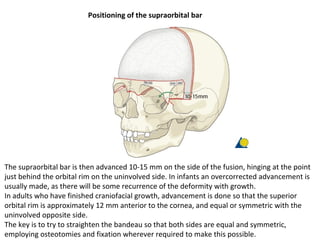
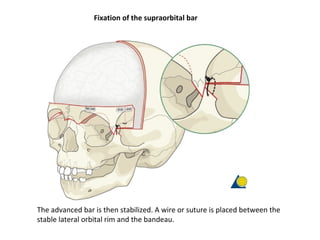
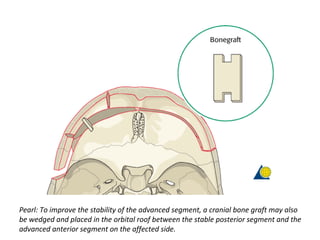
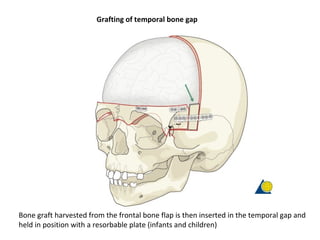
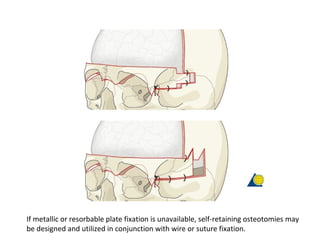
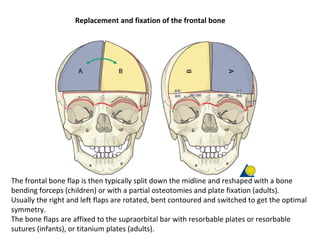
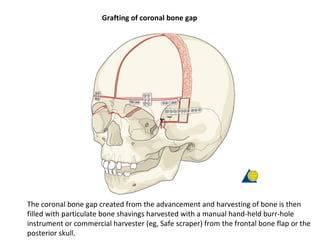
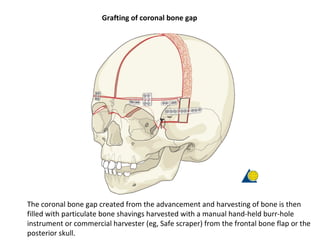
A bifrontal craniotomy is performed to remove the frontal bone. The supraorbital bar is advanced 10-15 mm and stabilized with wires or sutures. Bone grafts from the frontal bone flap are used to fill gaps in the temporal area and coronal bone. The frontal bone flap is reshaped and reattached with plates or sutures.