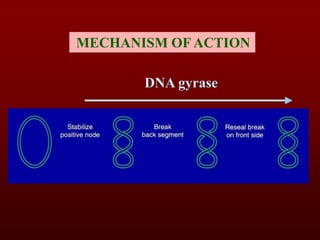
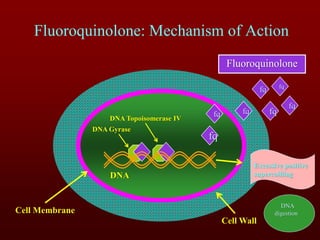
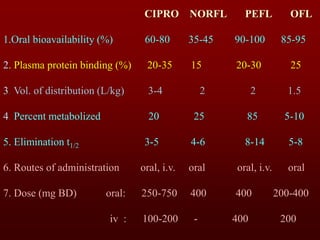
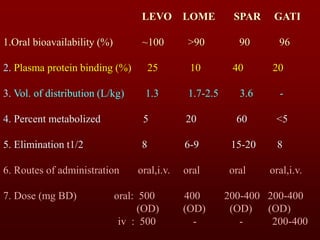
The document outlines the competencies and learning objectives regarding fluoroquinolones, detailing their antibacterial spectrum, mechanism of action, resistance, clinical uses, and adverse effects. It categorizes fluoroquinolones into first and second generations, discusses their pharmacokinetics, and lists specific examples along with their applications in various infections. The document also addresses benefits, resistance mechanisms, and potential drug interactions associated with fluoroquinolones.