
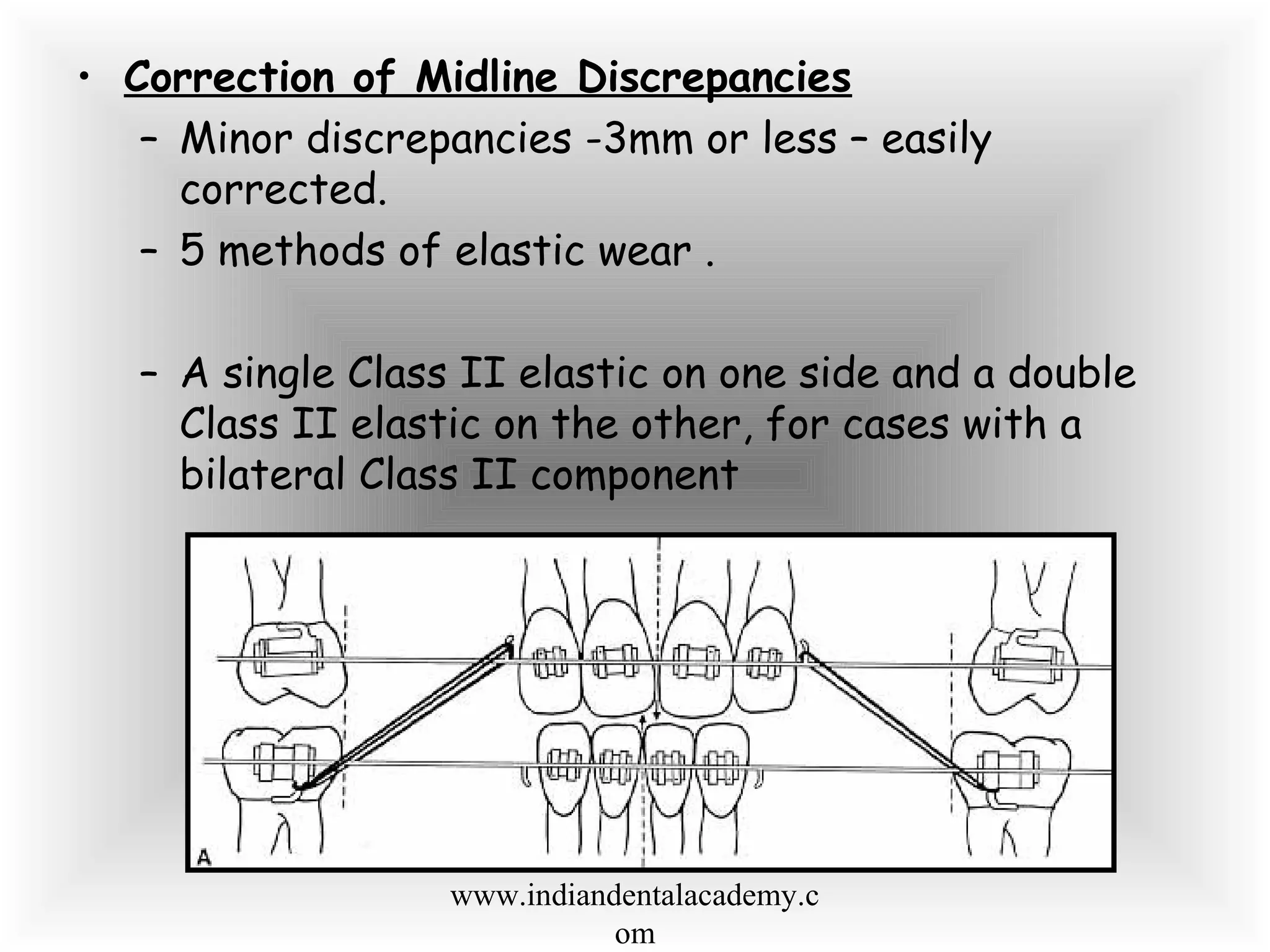
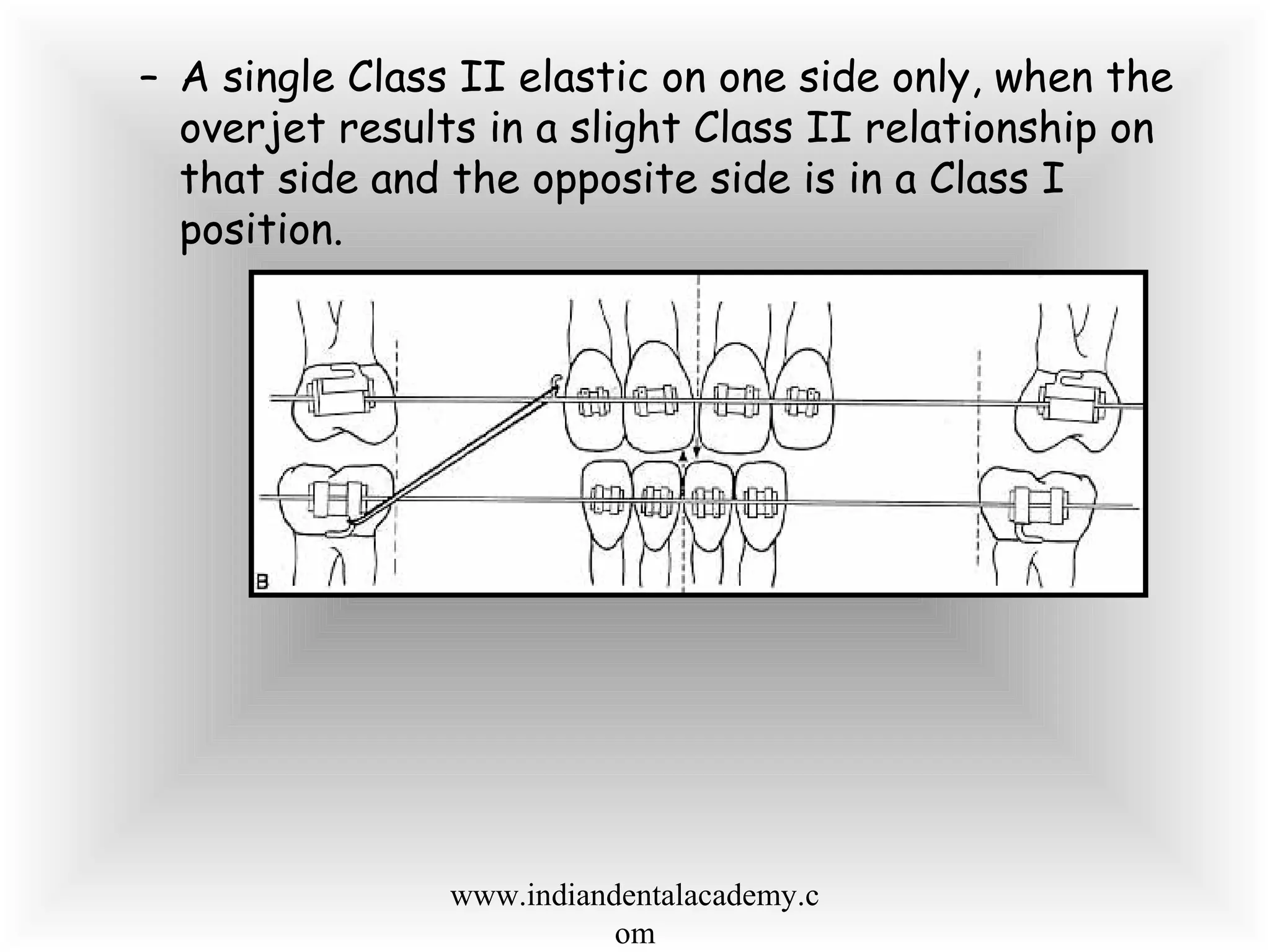
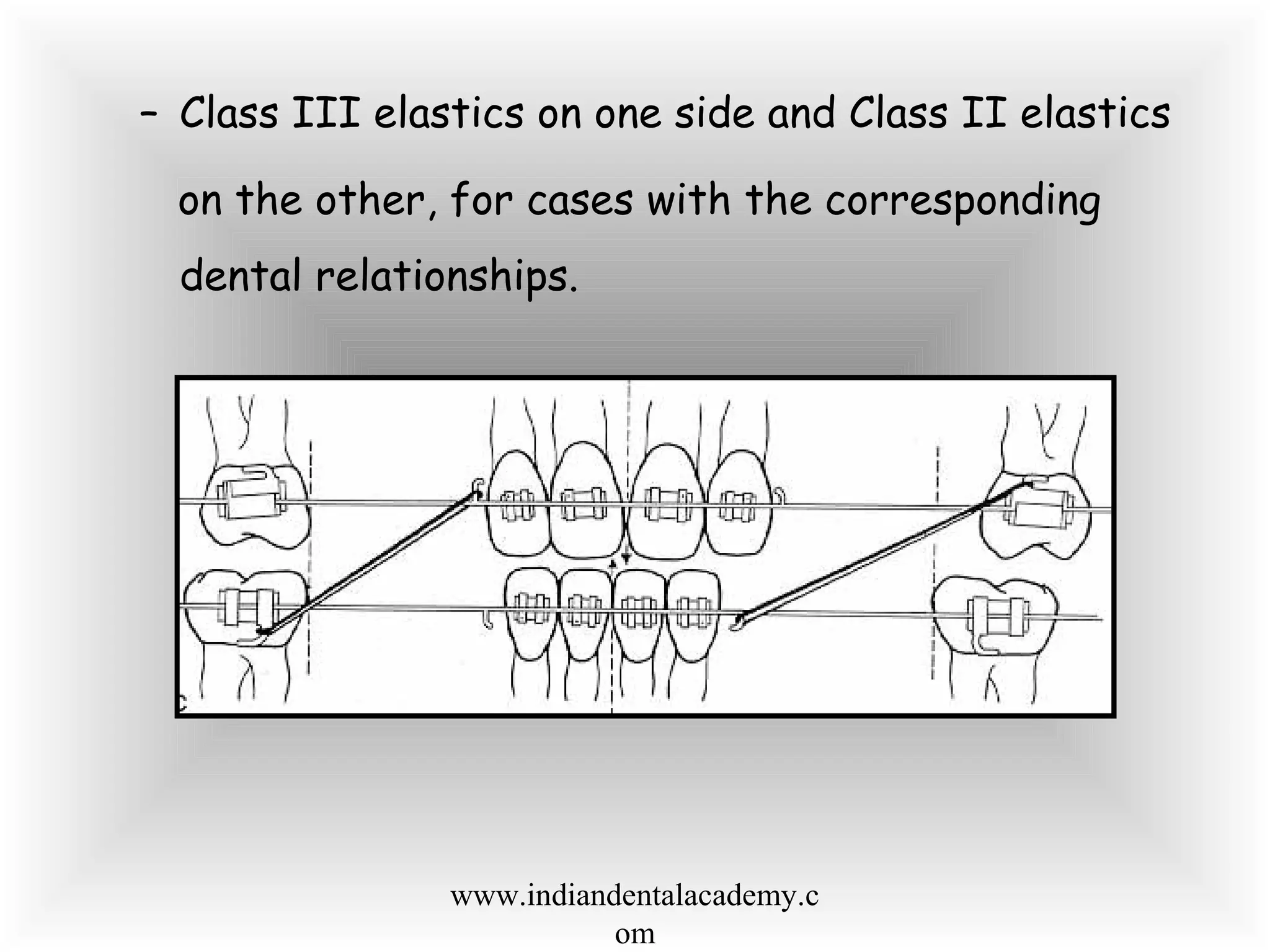
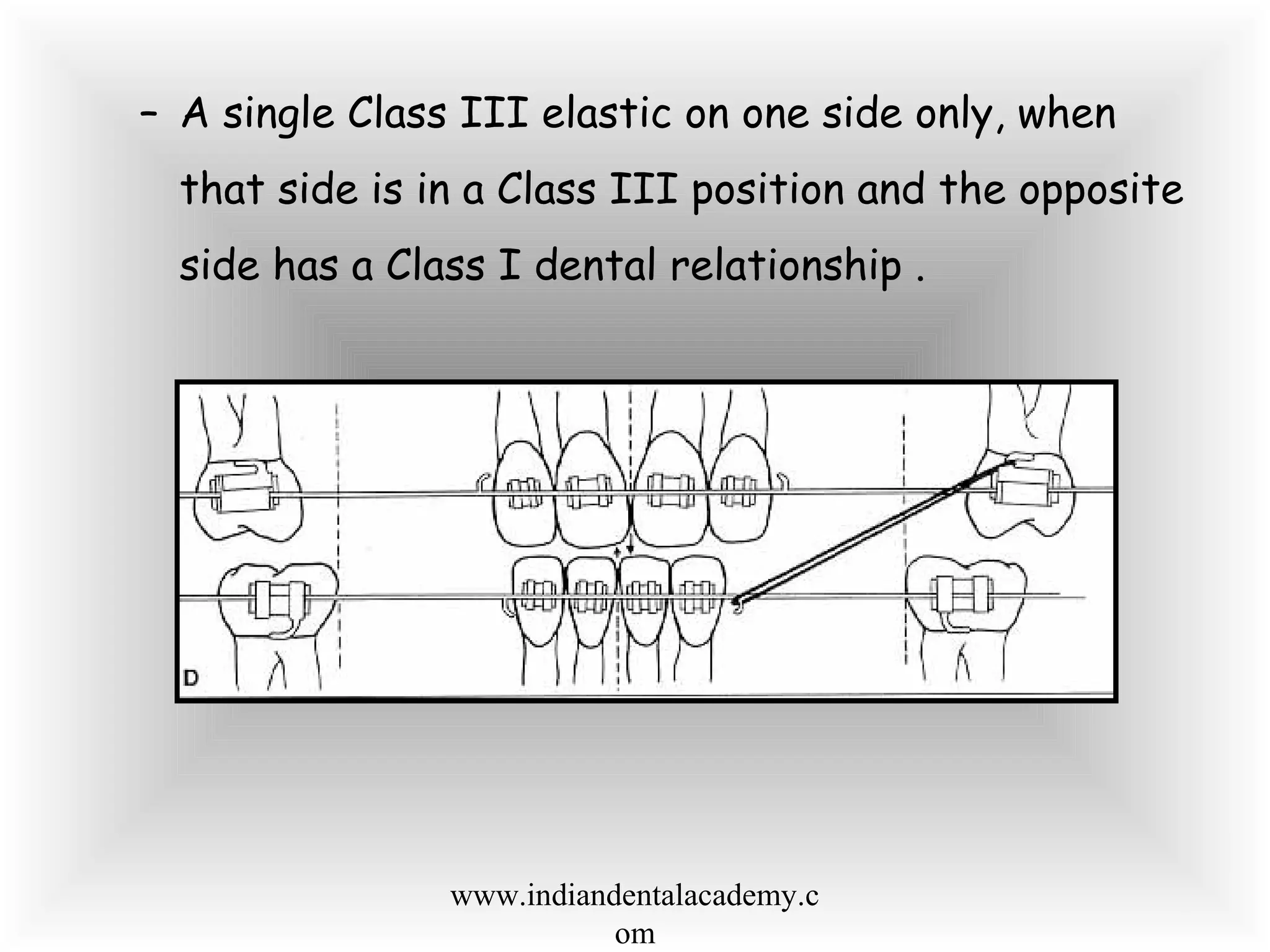
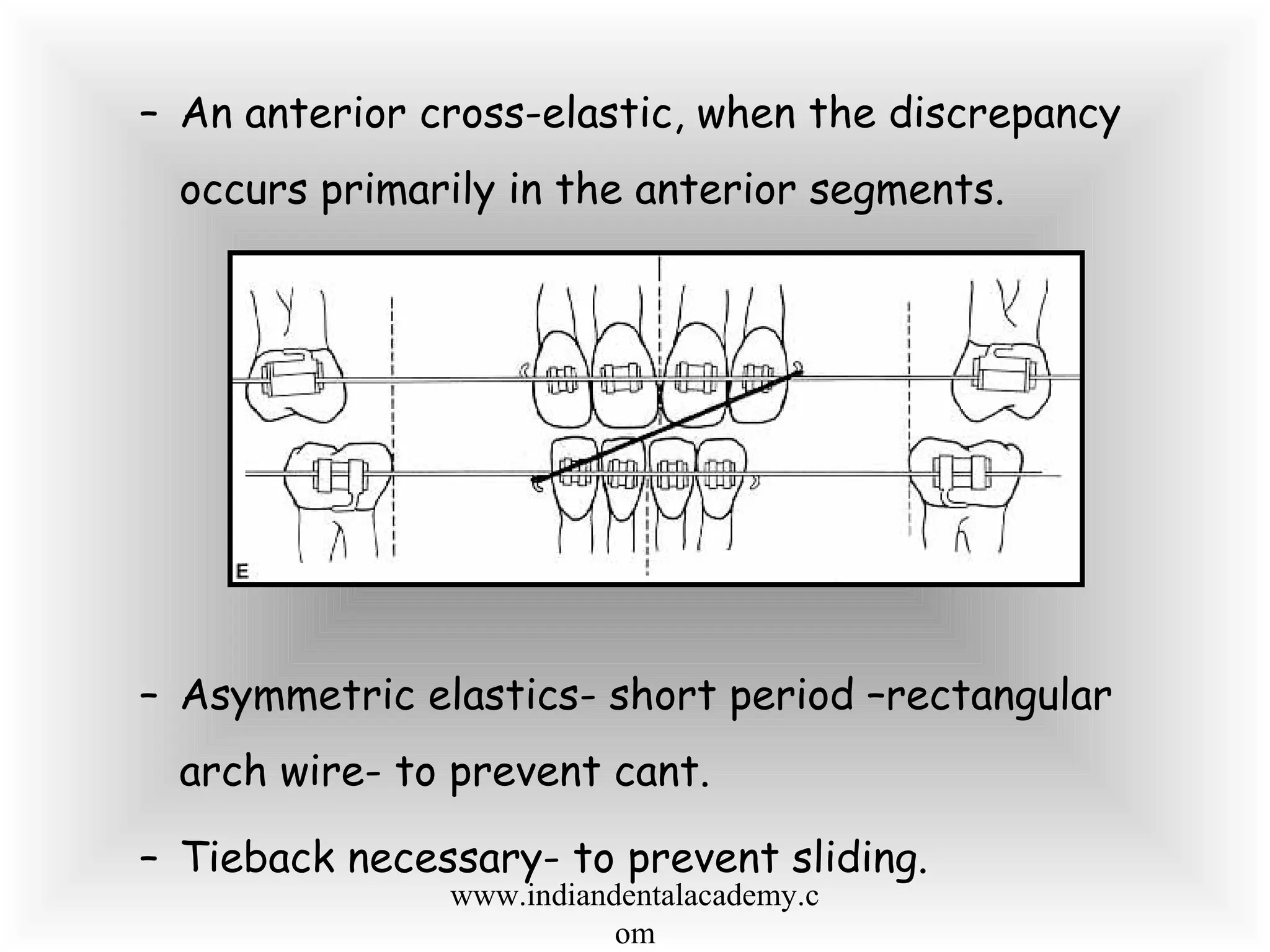
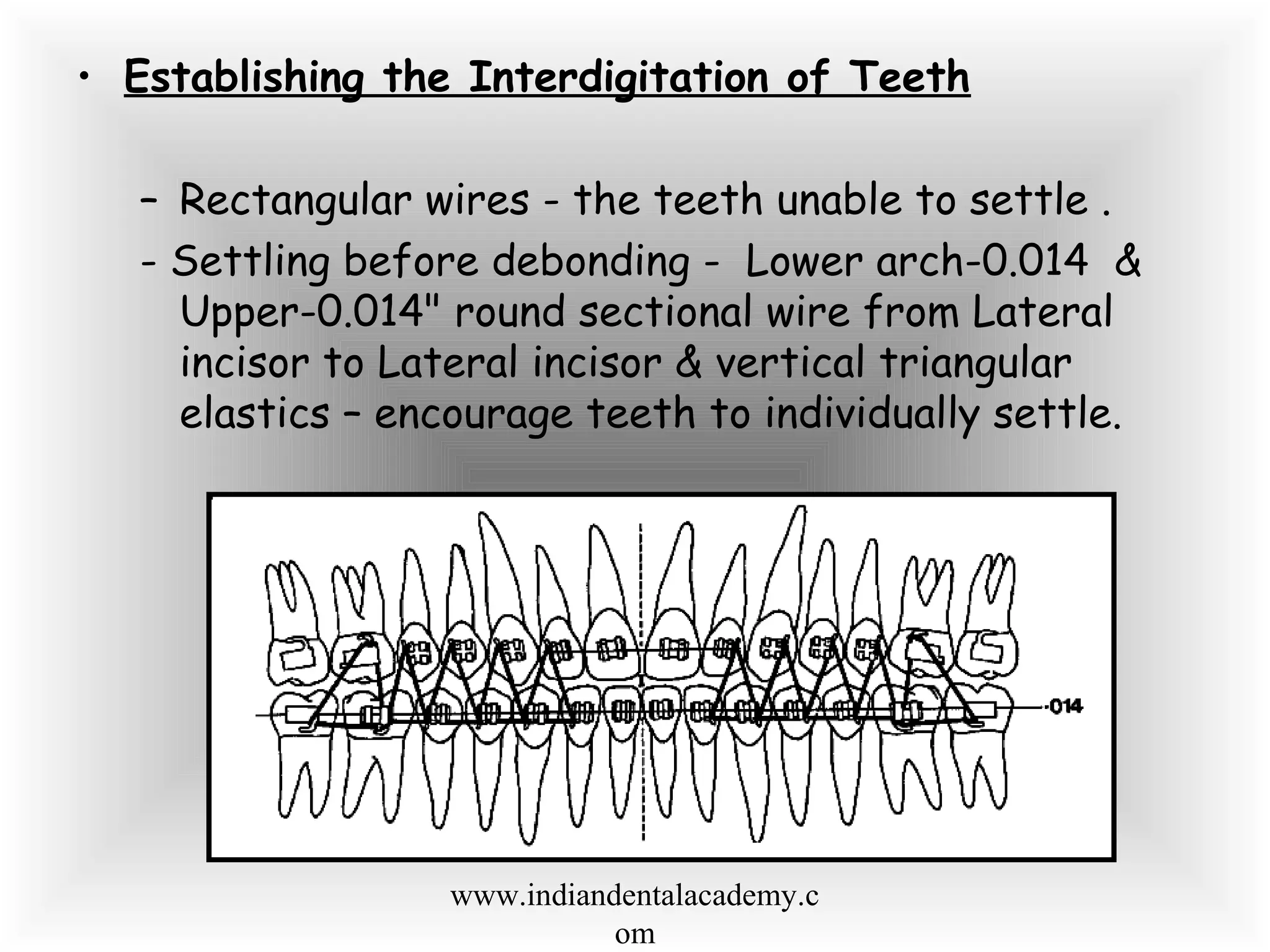

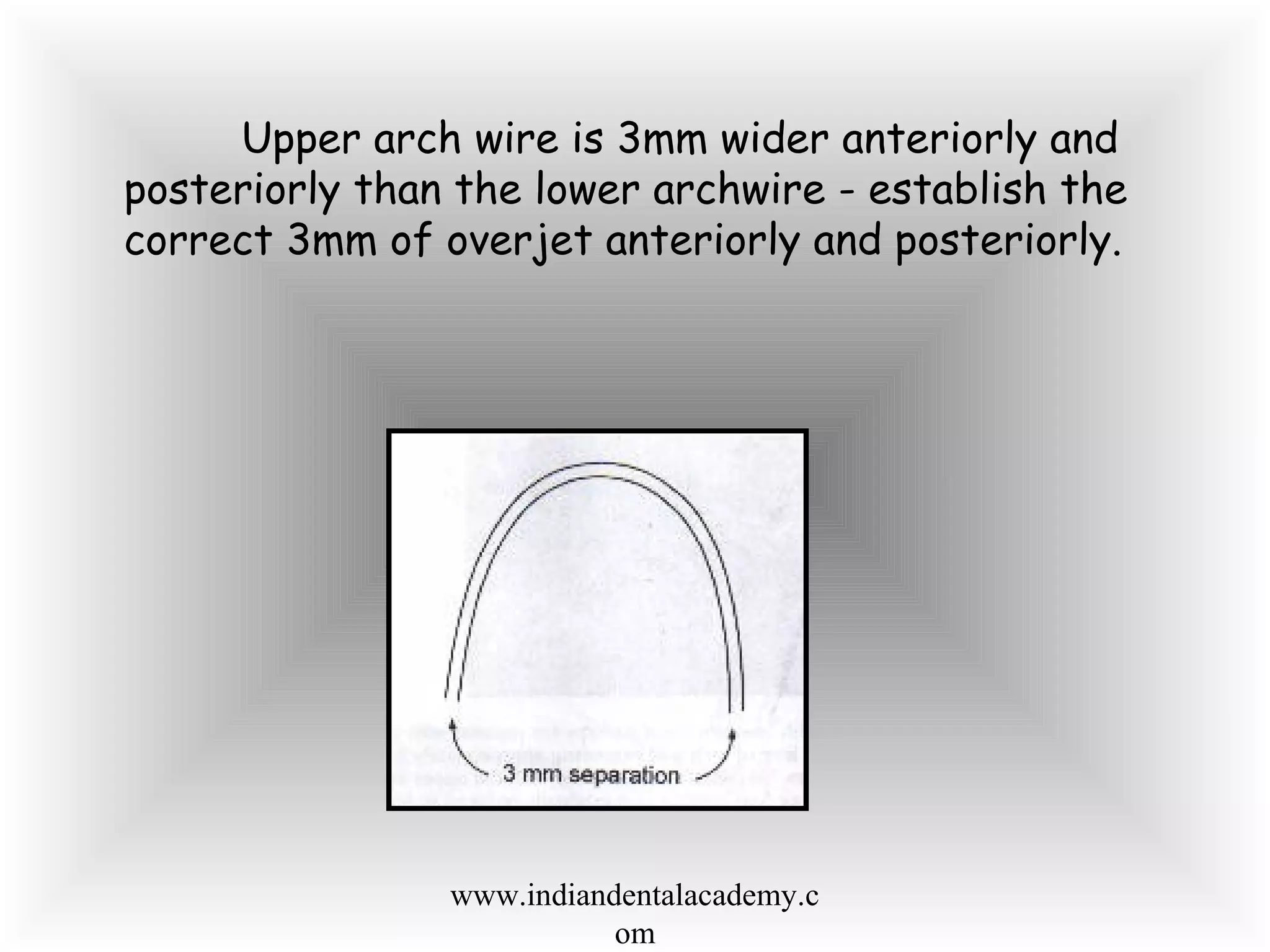
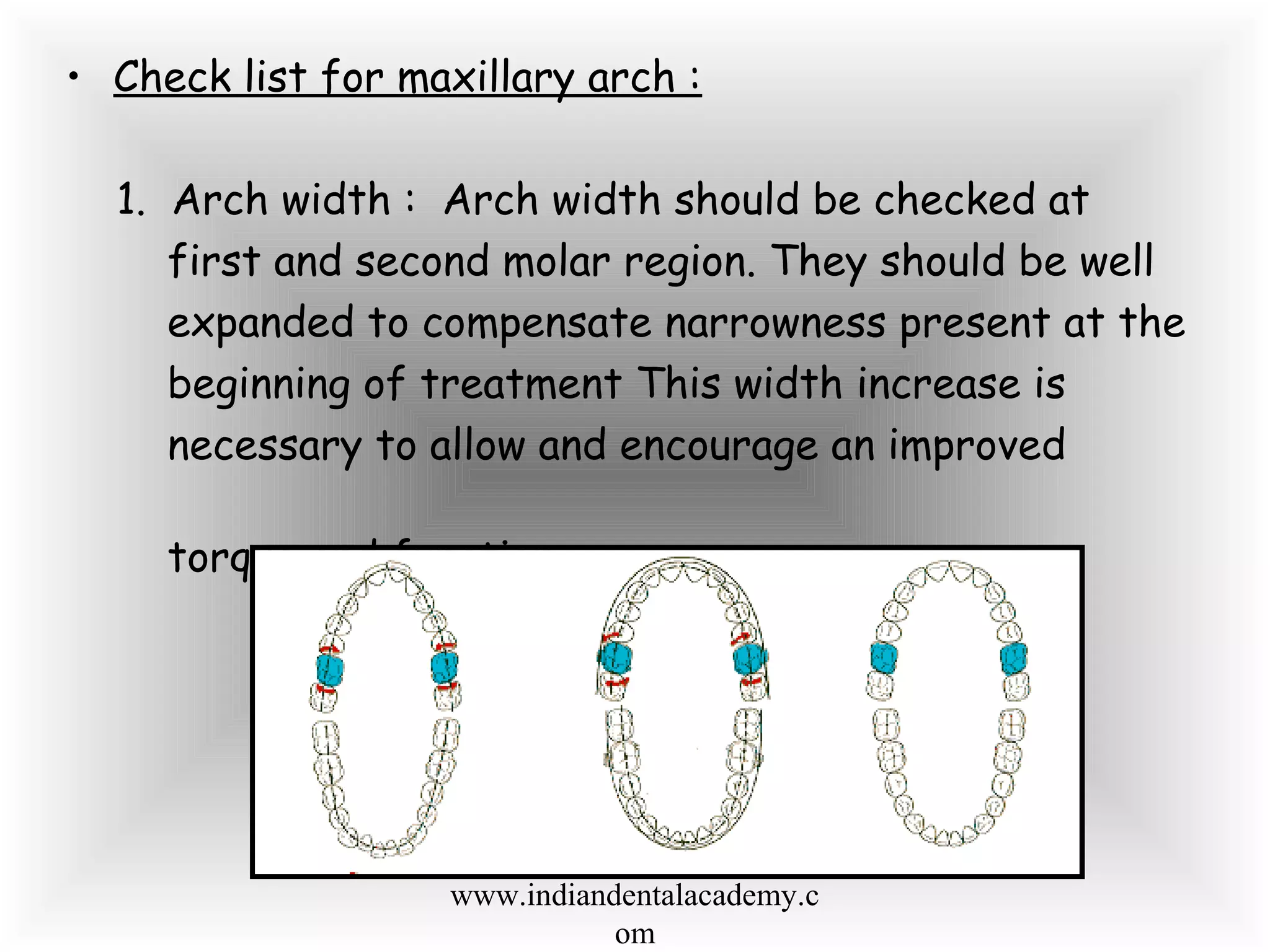
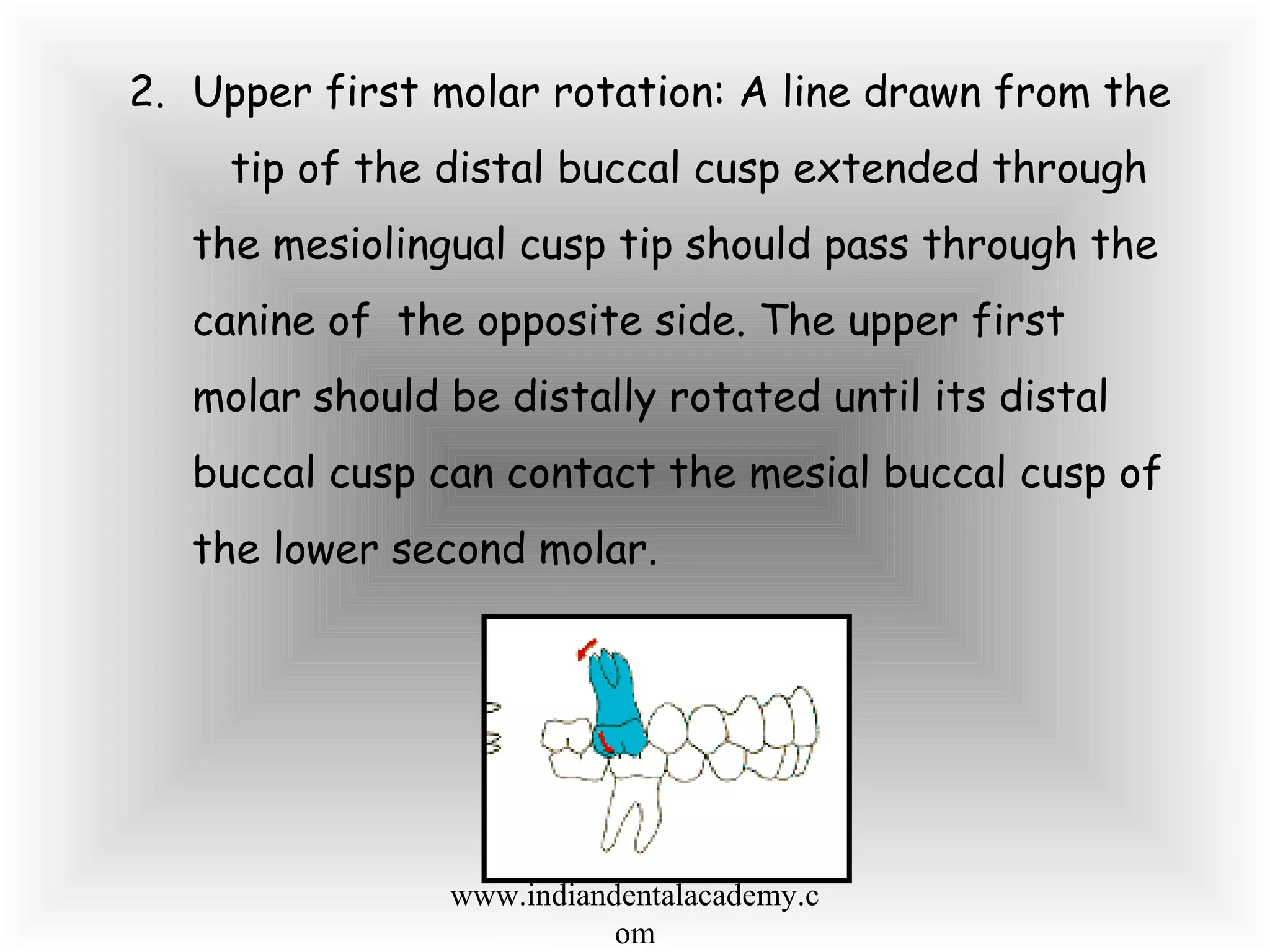

The document outlines the processes of finishing and detailing in orthodontic treatment, emphasizing the importance of achieving ideal tooth positioning for optimal stability, aesthetics, and periodontal health. It details various treatment goals, techniques for correcting tooth positions, and the adjustment of braces to achieve desired outcomes, including considerations for torque, midline discrepancies, and maintaining proper occlusal relationships. Additionally, it discusses factors such as cephalometric objectives and the evaluation of functional movements and TMJ dysfunction during the final stages of orthodontic treatment.























































































