Definition
• Fertilization isthe process by which a male gamete (spermatozoon) fuses with a female
gamete (oocyte) to form a diploid zygote, initiating embryonic development.
• It normally occurs in the ampulla of the fallopian tube within 24 hours of ovulation.
3.
Preparatory Events BeforeFertilization
A. Capacitation of Sperm
• Definition: Functional maturation of sperm after entering the female reproductive tract.
• Duration: ~7 hours.
• Changes:
➢ Removal of glycoprotein coat and seminal plasma proteins from sperm membrane.
➢ Increased membrane fluidity and calcium influx.
➢ Enhanced motility and ability to undergo acrosome reaction.
• Site: Uterus & fallopian tubes.
4.
B. Acrosome Reaction
•Triggered when capacitated sperm contacts the zona pellucida of the oocyte (specifically
ZP3 glycoprotein).
• Fusion of the sperm plasma membrane with the outer acrosomal membrane → release of
enzymes (hyaluronidase, acrosin).
• Enzymes digest zona pellucida → sperm penetrates.
5.
Stages of Fertilization
Step1: Approach of Sperm to the Oocyte
• Millions of sperm are deposited in the vagina during ejaculation.
• Only a few hundred reach the ampulla.
• Sperm swim using flagellar movement and are guided by chemotaxis and thermotaxis.
Step 2: Penetration of the Corona Radiata
• Corona radiata: Outer layer of follicular cells surrounding the oocyte.
• Hyaluronidase from sperm and motility help disperse cells.
Step 3: Binding to the Zona Pellucida
• Sperm binds to ZP3 receptors on zona pellucida.
• Binding triggers the acrosome reaction.
6.
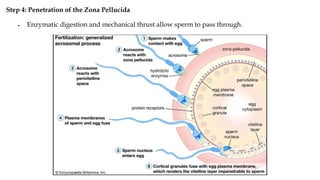
Step 4: Penetrationof the Zona Pellucida
• Enzymatic digestion and mechanical thrust allow sperm to pass through.
7.
Step 5: Fusionof Sperm and Oocyte Membranes
• Sperm’s plasma membrane fuses with oocyte’s plasma membrane (oolemma).
• Sperm head and tail enter the oocyte cytoplasm; the plasma membrane of sperm remains
outside.
Step 6: Cortical Reaction (Block to Polyspermy)
• Oocyte releases cortical granules into perivitelline space.
• Zona pellucida becomes impenetrable to other sperm (zona reaction).
Step 7: Completion of Meiosis II by Oocyte
• Secondary oocyte (arrested in metaphase II) completes meiosis after sperm entry.
• Forms mature ovum and second polar body.
8.
Step 8: Formationof Male and Female Pronuclei
• Sperm nucleus decondenses → male pronucleus.
• Oocyte nucleus forms female pronucleus.
• Both replicate DNA in preparation for mitosis.
Step 9: Fusion of Pronuclei (Syngamy)
• Nuclear envelopes dissolve; chromosomes intermingle.
• Diploid zygote (46 chromosomes) is formed.
9.
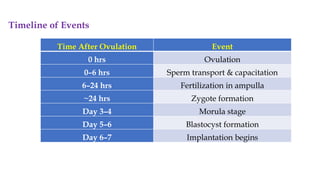
Timeline of Events
TimeAfter Ovulation Event
0 hrs Ovulation
0–6 hrs Sperm transport & capacitation
6–24 hrs Fertilization in ampulla
~24 hrs Zygote formation
Day 3–4 Morula stage
Day 5–6 Blastocyst formation
Day 6–7 Implantation begins
10.
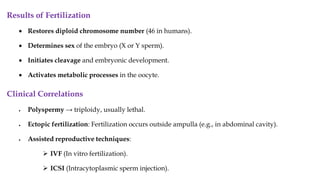
Results of Fertilization
•Restores diploid chromosome number (46 in humans).
• Determines sex of the embryo (X or Y sperm).
• Initiates cleavage and embryonic development.
• Activates metabolic processes in the oocyte.
Clinical Correlations
• Polyspermy → triploidy, usually lethal.
• Ectopic fertilization: Fertilization occurs outside ampulla (e.g., in abdominal cavity).
• Assisted reproductive techniques:
➢ IVF (In vitro fertilization).
➢ ICSI (Intracytoplasmic sperm injection).
11.
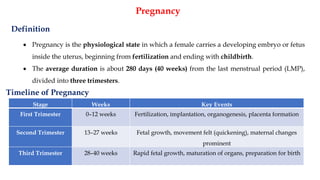
Pregnancy
Definition
• Pregnancy isthe physiological state in which a female carries a developing embryo or fetus
inside the uterus, beginning from fertilization and ending with childbirth.
• The average duration is about 280 days (40 weeks) from the last menstrual period (LMP),
divided into three trimesters.
Stage Weeks Key Events
First Trimester 0–12 weeks Fertilization, implantation, organogenesis, placenta formation
Second Trimester 13–27 weeks Fetal growth, movement felt (quickening), maternal changes
prominent
Third Trimester 28–40 weeks Rapid fetal growth, maturation of organs, preparation for birth
Timeline of Pregnancy
12.
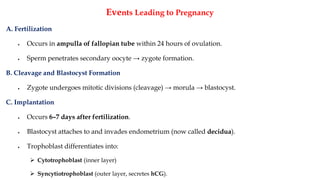
Events Leading toPregnancy
A. Fertilization
• Occurs in ampulla of fallopian tube within 24 hours of ovulation.
• Sperm penetrates secondary oocyte → zygote formation.
B. Cleavage and Blastocyst Formation
• Zygote undergoes mitotic divisions (cleavage) → morula → blastocyst.
C. Implantation
• Occurs 6–7 days after fertilization.
• Blastocyst attaches to and invades endometrium (now called decidua).
• Trophoblast differentiates into:
➢ Cytotrophoblast (inner layer)
➢ Syncytiotrophoblast (outer layer, secretes hCG).
14.
Development of Placenta
•Placenta forms from fetal chorion and maternal decidua basalis.
• Functions:
➢ Exchange of nutrients, gases, wastes.
➢ Hormone secretion (hCG, progesterone, estrogens, human placental lactogen).
Hormonal Changes in Pregnancy
• hCG: Maintains corpus luteum in early pregnancy; peaks at ~10 weeks.
• Progesterone: Maintains endometrial lining, inhibits uterine contractions.
• Estrogen: Promotes uterine growth, breast development.
• Human placental lactogen (hPL): Alters maternal metabolism for fetal nutrition.
• Relaxin: Softens ligaments and cervix.
15.
Physiological Changes inthe Mother
A. Cardiovascular System
• Blood volume ↑ 30–50%, Cardiac output ↑, Heart rate ↑ ~10–15 bpm.
B. Respiratory System
• Tidal volume ↑, Oxygen consumption ↑.
C. Renal System
• Glomerular filtration rate (GFR) ↑, Increased urinary frequency.
D. Gastrointestinal System
• Decreased motility (due to progesterone) → constipation, reflux.
E. Musculoskeletal System
• Relaxation of pelvic ligaments, Shift in center of gravity → lumbar lordosis.
16.
Stages of FetalDevelopment
First Trimester
• Organogenesis completed by week 8.
• Embryo → fetus by week 9.
• High risk of teratogenic effects.
Second Trimester
• Fetal movements felt (quickening ~18–20 weeks in first pregnancy, earlier in later ones).
• Sex determination possible via ultrasound.
Third Trimester
• Lungs mature.
• Fat deposition under skin.
• Fetus positions for birth.
17.
Clinical Signs ofPregnancy
Presumptive Signs (subjective)
• Amenorrhea, Morning sickness, Breast tenderness.
Probable Signs (objective)
• Positive pregnancy test (hCG in urine/blood), Enlarged uterus, Hegar’s sign (softening of
uterus).
Positive Signs
• Fetal heart sounds (Doppler), Ultrasound visualization of fetus, Palpation of fetal parts.
18.
Diagnosis
• Urine pregnancytest: Detects hCG.
• Ultrasound: Confirms gestational sac and fetal heartbeat.
Common Discomforts in Pregnancy
• Nausea/vomiting, Backache, Leg cramps, Edema, Heartburn.
Complications of Pregnancy
• Hypertensive disorders (e.g., preeclampsia), Gestational diabetes, Placenta previa / placental abruption,
Preterm labor.
Termination of Pregnancy
• Normal delivery: Vaginal birth.
• Cesarean section: Surgical delivery.
• Preterm: Birth before 37 weeks.
• Post-term: Birth after 42 weeks.
19.
Parturition
Definition
• Parturition isthe physiological process by which the fetus, placenta, and fetal membranes are
expelled from the mother’s uterus at the end of pregnancy.
• It usually occurs around 38–40 weeks of gestation in humans
21.
Initiation of Parturition
•Parturition is triggered by a complex interaction between fetal maturity signals and maternal
hormonal changes.
A. Fetal Factors
• Fetal adrenal glands secrete cortisol, which:
➢ Increases placental estrogen production.
➢ Stimulates prostaglandin synthesis.
• Fetal lung maturity: Secretion of surfactant proteins (especially SP-A) also signals readiness for
birth.
B. Maternal Factors
• Stretching of the uterus and cervix stimulates neuroendocrine reflexes.
• Increasing estrogen levels near term enhance myometrial sensitivity to oxytocin.
22.
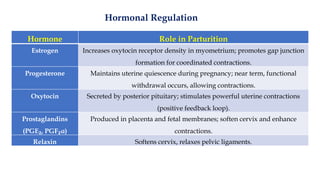
Hormone Role inParturition
Estrogen Increases oxytocin receptor density in myometrium; promotes gap junction
formation for coordinated contractions.
Progesterone Maintains uterine quiescence during pregnancy; near term, functional
withdrawal occurs, allowing contractions.
Oxytocin Secreted by posterior pituitary; stimulates powerful uterine contractions
(positive feedback loop).
Prostaglandins
(PGE₂, PGF₂α)
Produced in placenta and fetal membranes; soften cervix and enhance
contractions.
Relaxin Softens cervix, relaxes pelvic ligaments.
Hormonal Regulation
23.
Positive Feedback Mechanism
•Uterine contractions push the fetal head against the cervix.
• Cervical stretch activates sensory impulses to hypothalamus.
• Posterior pituitary releases oxytocin.
• Oxytocin intensifies uterine contractions.
• More cervical stretch → more oxytocin (cycle continues until birth).
24.
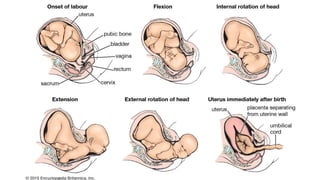
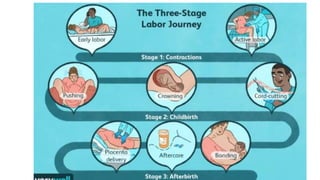
Stages of Labor
•Parturition is divided into three stages:
Stage 1: Cervical Dilation
• Duration: Longest stage (6–12 hours in first pregnancy, shorter in later ones), Regular uterine
contractions begin, Cervix effaces (thins) and dilates to ~10 cm, Amniotic sac may rupture
(“water breaks”).
Stage 2: Expulsion of the Baby
• Duration: 30–120 minutes (shorter in multiparas), From full cervical dilation to delivery of
baby, Powerful contractions aided by maternal pushing efforts, Ends with birth of the infant.
Stage 3: Placental Delivery
• Duration: 5–30 minutes after birth, Uterus contracts to expel placenta and membranes, Helps
prevent postpartum hemorrhage by compressing blood vessels.
26.
Maternal Changes AfterParturition
• Uterine involution: Uterus gradually shrinks to pre-pregnancy size within ~6 weeks.
• Lochia: Vaginal discharge (blood, mucus, uterine tissue) for 4–6 weeks.
• Hormonal changes: Estrogen and progesterone levels drop sharply; prolactin remains high for
lactation.
Clinical Significance
• Preterm labor: Parturition before 37 weeks; risk for neonatal complications.
• Prolonged labor: Labor lasting >20 hours (first-time mothers) or >14 hours (multiparas).
• Obstructed labor: Baby cannot pass through birth canal → may require C-section.
• Postpartum hemorrhage: Excessive bleeding after delivery.





































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)