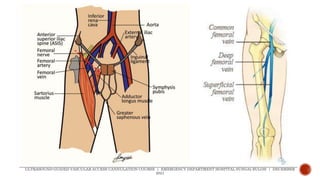
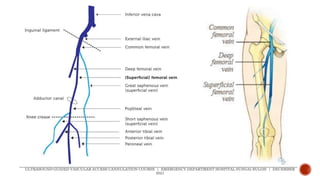
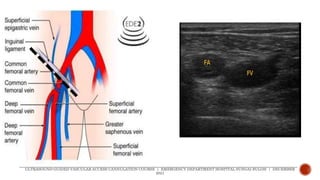
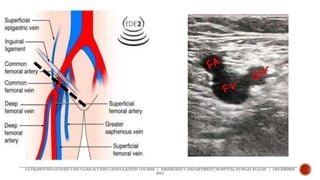
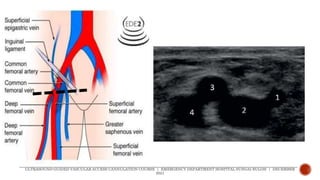
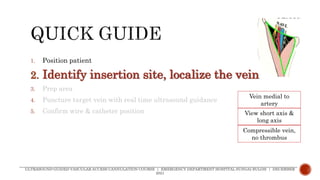
This document provides information on ultrasound-guided femoral vein cannulation. It discusses the advantages and disadvantages of the procedure, as well as contraindications. Key steps of the procedure are outlined, including patient positioning, identifying the vein with ultrasound, needle puncture under real-time ultrasound guidance, and confirming wire and catheter placement. Anatomy of the femoral vein and artery is described. Potential complications are also noted. The goal of the document is to provide guidance on performing femoral vein cannulation safely and effectively using ultrasound.