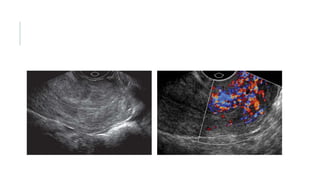
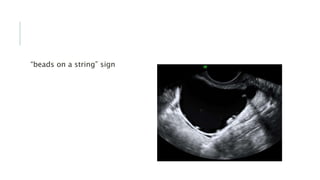
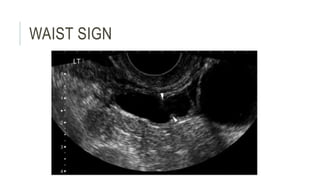
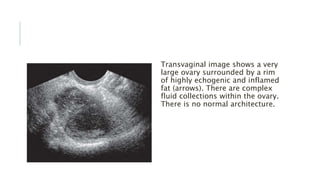
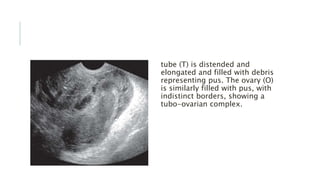
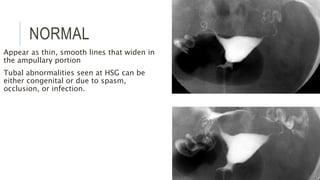
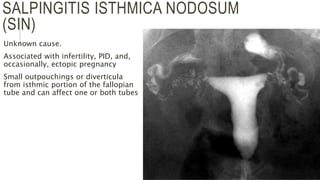
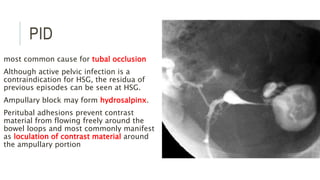
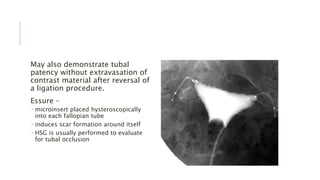
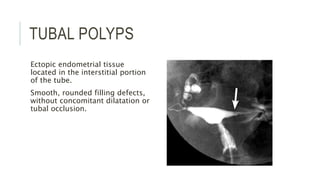
The fallopian tubes are normally difficult to see on imaging unless dilated or filled with fluid. Common abnormalities include infections like pelvic inflammatory disease which can cause tubal blockage and adhesions. Imaging findings of PID include thickened tubal walls and signs of inflammation. Tubo-ovarian complexes with septations may form from infections. Rare tumors can also involve the fallopian tubes. Hysterosalpingography is commonly used to evaluate the fallopian tubes and can reveal abnormalities from prior infections, surgeries, or conditions like salpingitis isthmica nodosa.