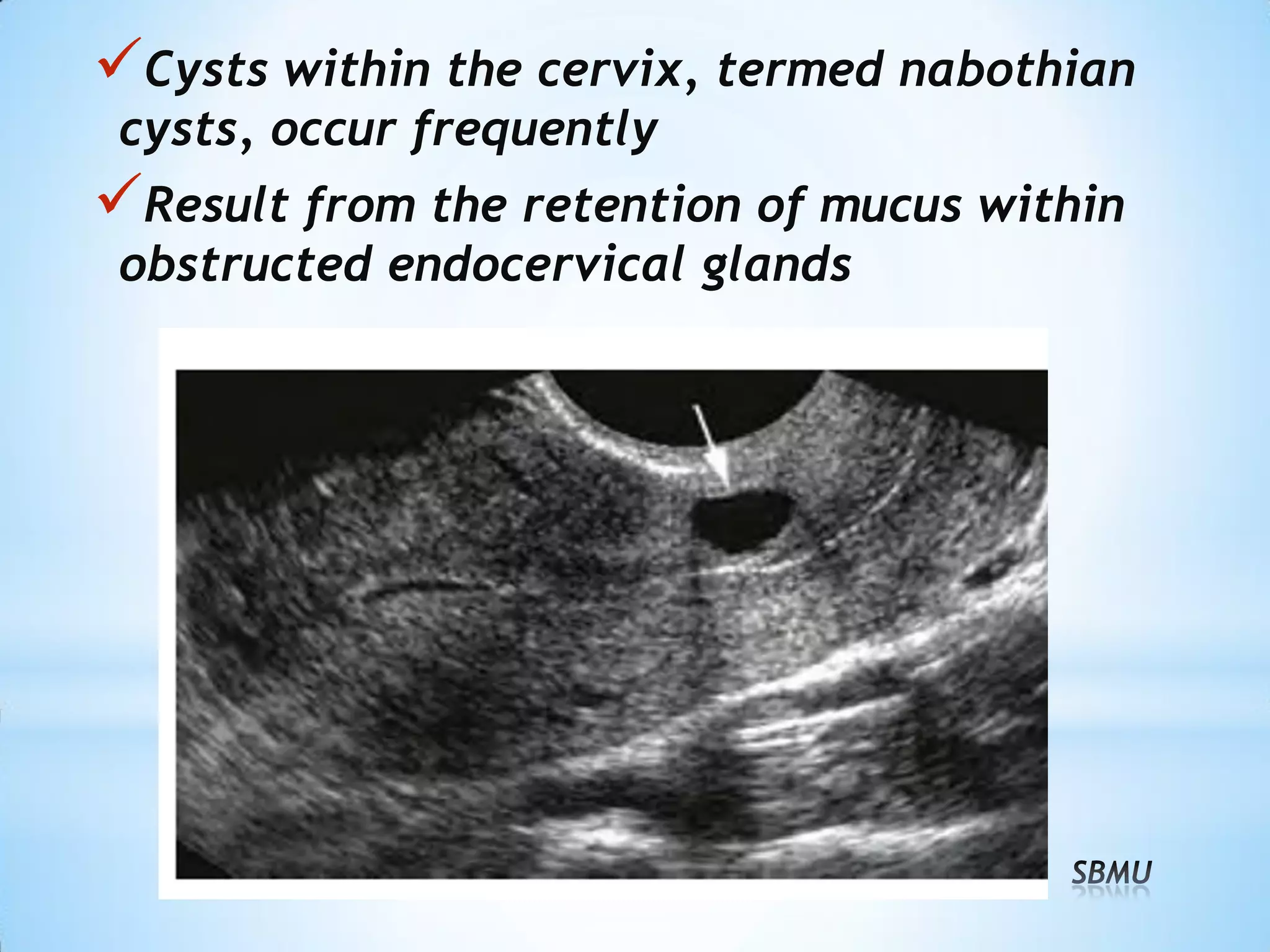
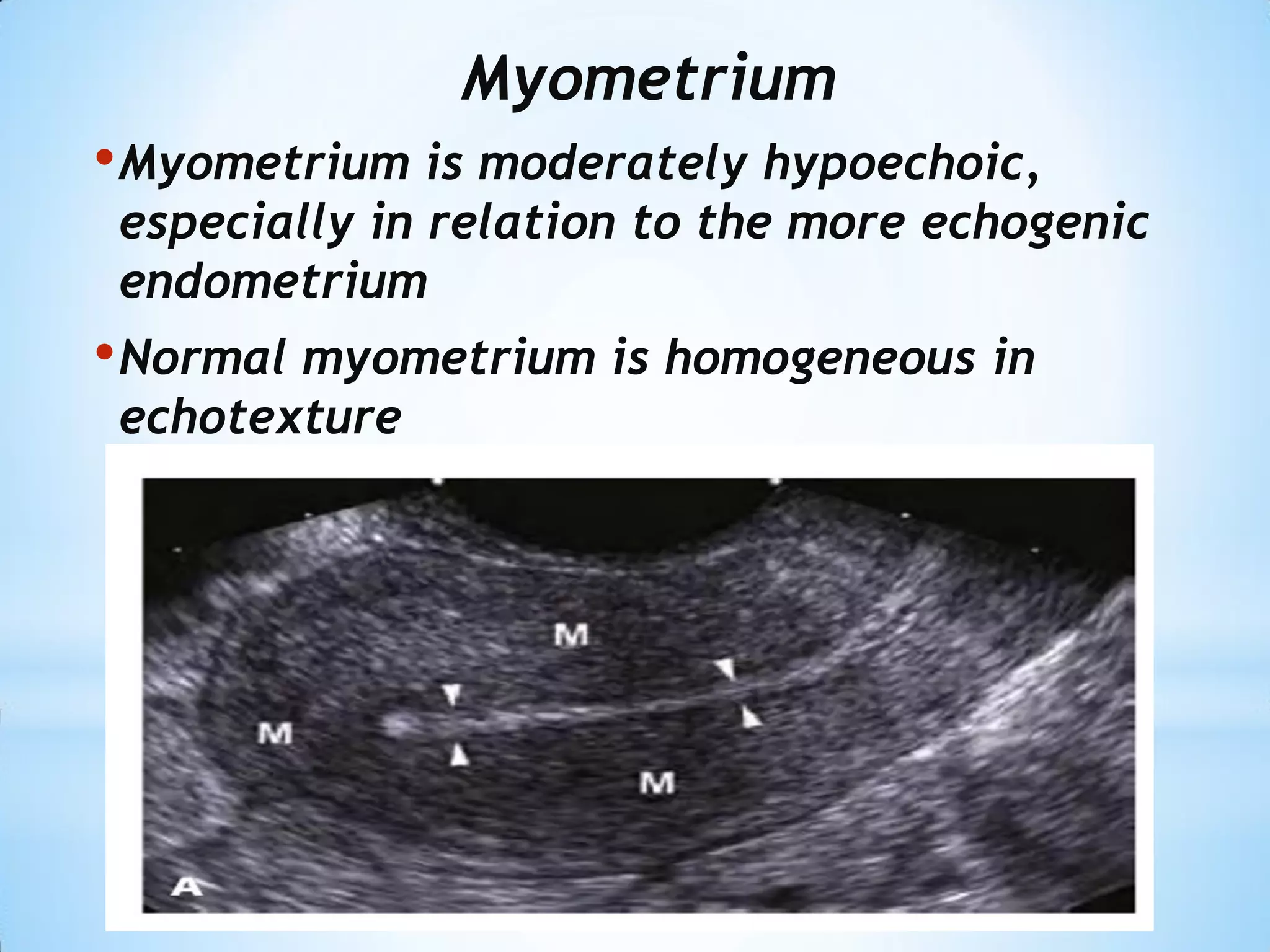
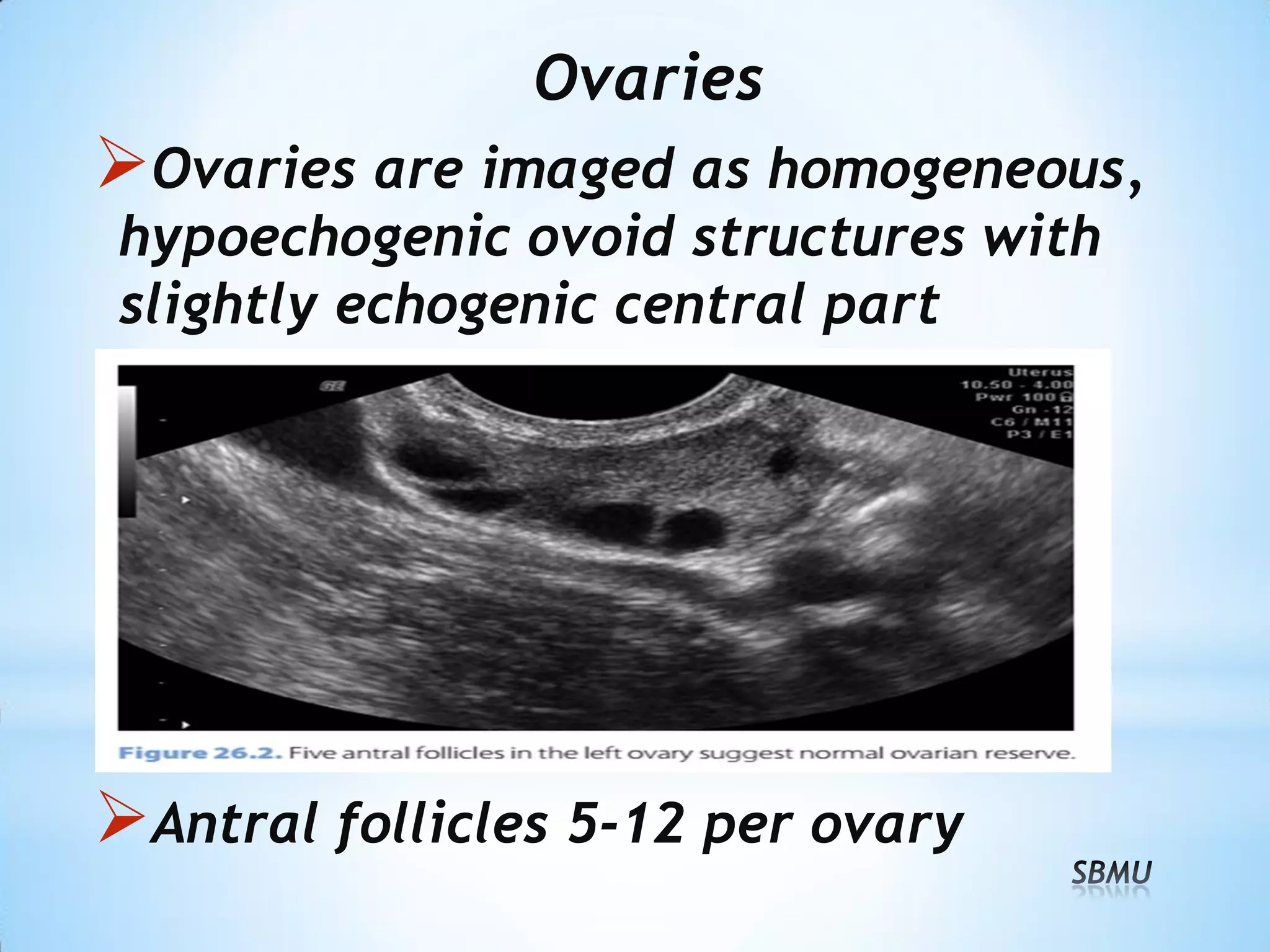
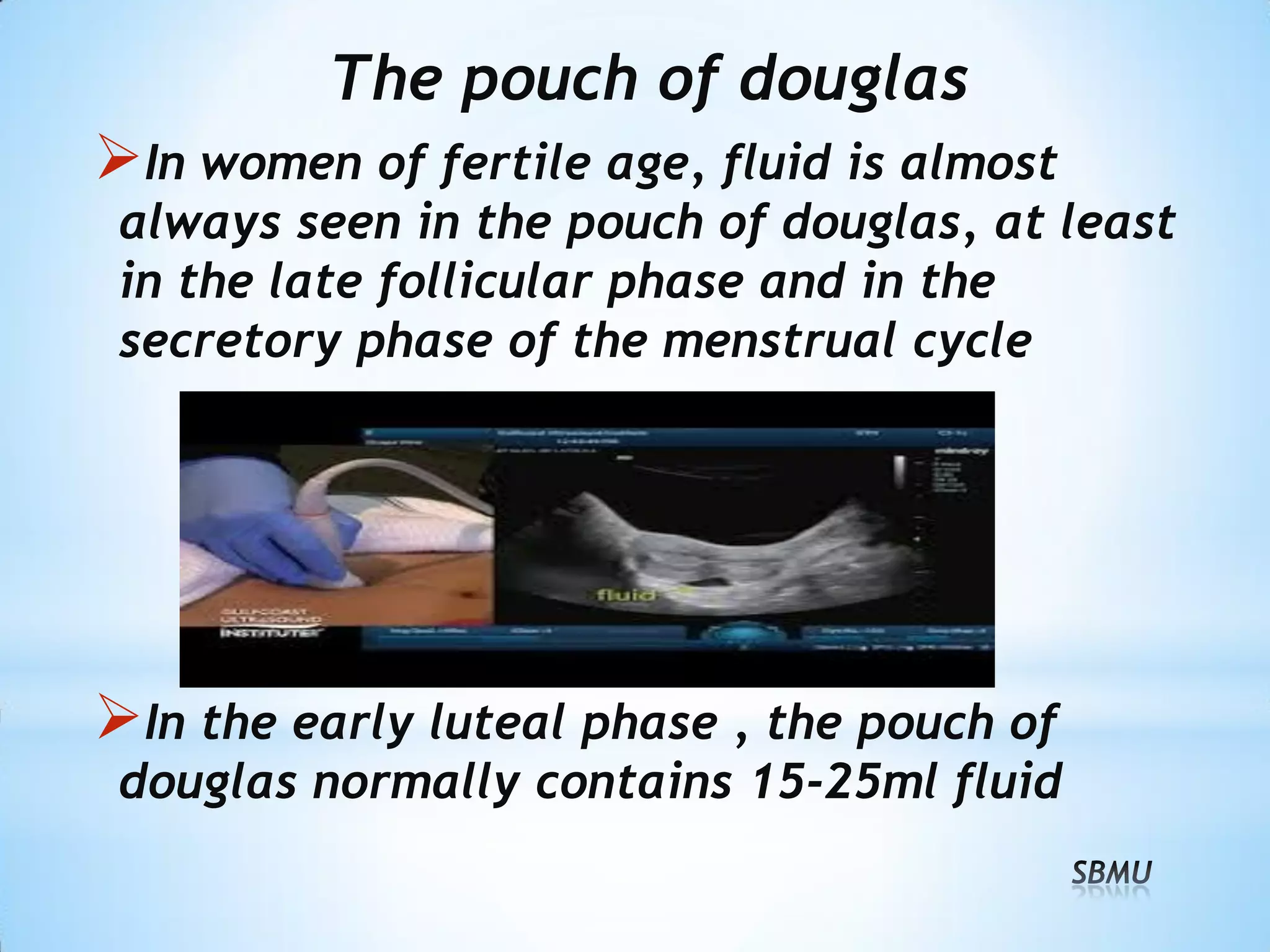
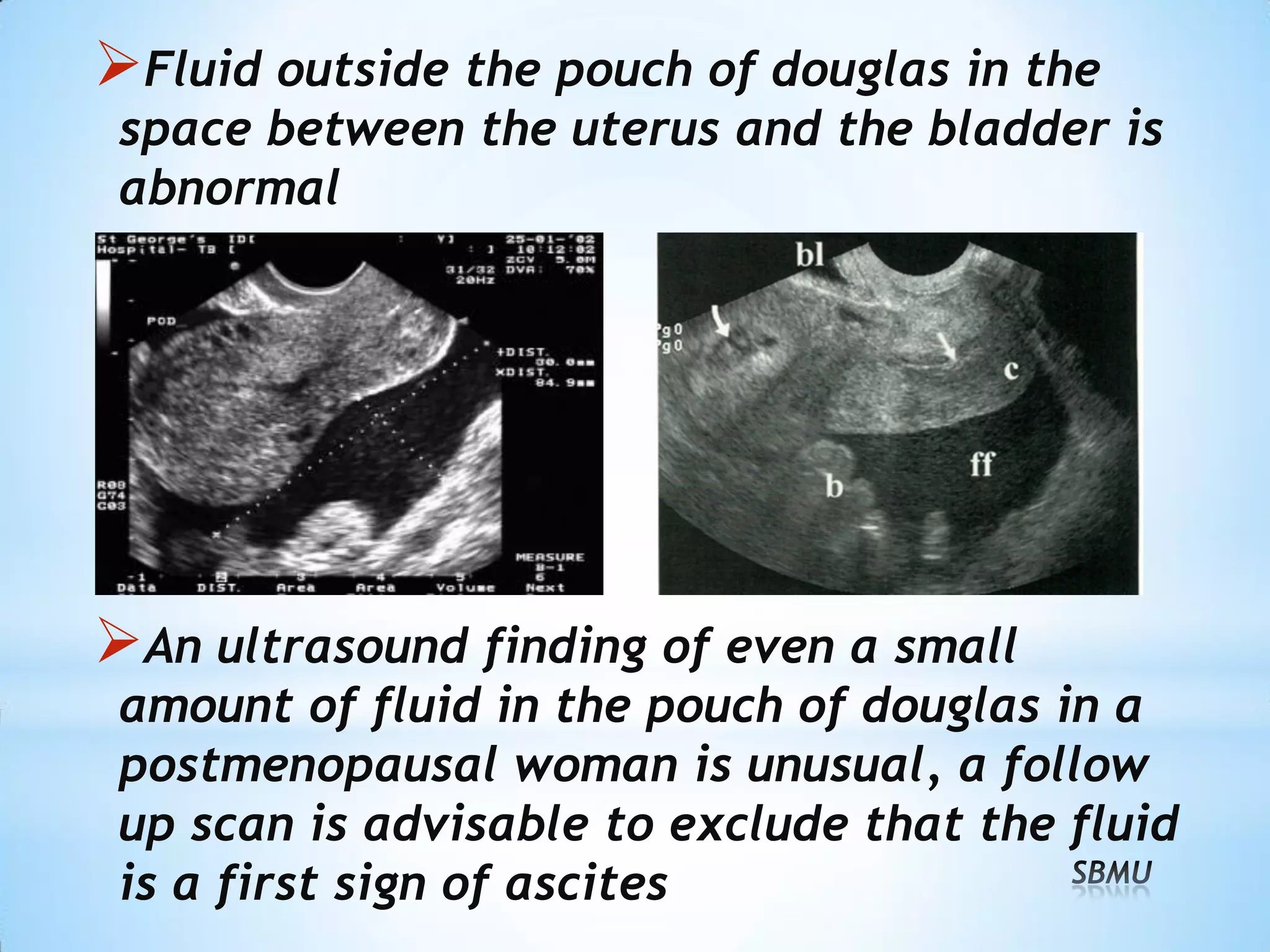
This document provides guidance on performing and interpreting a normal pelvic ultrasound exam. It reviews female pelvic anatomy including the uterus, endometrium, myometrium, ovaries, fallopian tubes, and pouch of Douglas. Exam preparation and approaches using transabdominal and transvaginal ultrasound are outlined. Key steps include reviewing the patient's history and symptoms, obtaining consent, and examining the uterus, ovaries, and other pelvic structures in both sagittal and coronal views to evaluate size, shape, echogenicity, and presence of any abnormalities. Fluid may normally be present in the pouch of Douglas but is abnormal elsewhere in the pelvis.