EMBRYOLOGY OF UTERUS
•The female reproductive tract develops from a pair of
Müllerian ducts that form the fallopian tubes, uterus,
cervix and the upper two-thirds of the vagina.
The ovaries and lower third of the vagina have a
different embryological origin (genital ridge and
urogenital sinus, respectively).
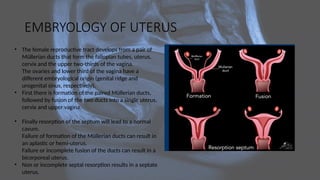
• First there is formation of the paired Müllerian ducts,
followed by fusion of the two ducts into a single uterus,
cervix and upper vagina.
• Finally resorption of the septum will lead to a normal
cavum.
Failure of formation of the Müllerian ducts can result in
an aplastic or hemi-uterus.
Failure or incomplete fusion of the ducts can result in a
bicorporeal uterus.
• Non or incomplete septal resorption results in a septate
uterus.
3.
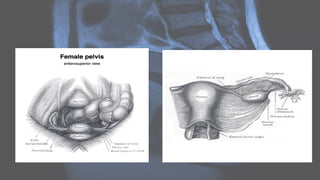
GROSS ANATOMY
• Theuterus is an hollow, thick-walled, muscular organ of the female
reproductive tract that lies in the lesser pelvis. The body of the uterus is
intraperitoneal and the cervix uteri is subperitoneal.
• The uterus has an inverted pear shape. It measures about 7.5 cm in
length, 5 cm wide at its upper part, and nearly 2.5 cm in thickness in
adults. It weighs approximately 30-40 g.
• The uterus is divisible into two portions: body and cervix. About midway
between the apex and base is a slight constriction known as the isthmus.
The portion above the isthmus is termed the body, and that below, the
cervix. The part of the body which lies above a plane passing through the
points of the entrance of the uterine tubes is known as the fundus.
4.
Relations
• anteriorly: bladder;uterovesical pouch
• posteriorly: rectum; pouch of Douglas
• laterally: broad ligament; round ligament; uterine vessels
• uterine tubes open into its upper part
• inferiorly: uterine cavity communicates with that of
the vagina.
6.
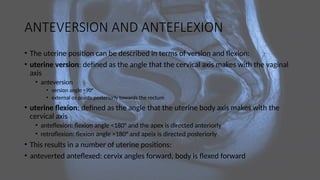
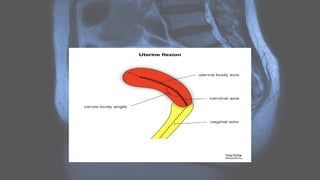
ANTEVERSION AND ANTEFLEXION
•The uterine position can be described in terms of version and flexion:
• uterine version: defined as the angle that the cervical axis makes with the vaginal
axis
• anteversion
• version angle <90°
• external os points posteriorly towards the rectum
• uterine flexion: defined as the angle that the uterine body axis makes with the
cervical axis
• anteflexion: flexion angle <180° and the apex is directed anteriorly
• retroflexion: flexion angle >180° and apeix is directed posteriorly
• This results in a number of uterine positions:
• anteverted anteflexed: cervix angles forward, body is flexed forward
8.
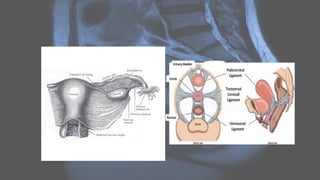
Attachments
Musculotendinous and ligamentousattachments:
• Anterior: pubocervical ligament
• Lateral: transverse cervical ligaments (cardinal or Mackenrodt’s)
• Posterior: uterosacral ligaments
• Inferior: puborectalis and pubovaginalis parts of the levator ani
muscle.
On CT
• Theuterus appears as a homogeneous soft tissue mass posterior to the
bladder. The myometrium shows low density on unenhanced CT with the
endometrial canal showing even lower density than myometrium . It normally
enhances post intravenous contrast.
• There are generally three types of enhancement in a normal uterus :
• type 1: thick or thin sub-endometrial enhancement, most commonly found in
pre-menopausal women
• type 2: diffuse myometrial enhancement, found in both pre and post-
menopausal women
• type 3: faint diffuse myometrial enhancement, exclusively found in post-
menopausal women
13.
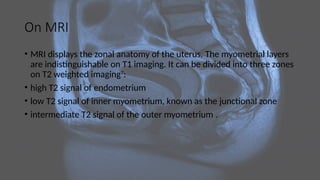
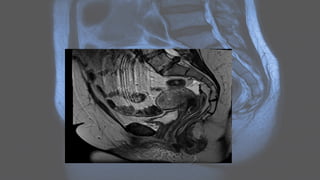
On MRI
• MRIdisplays the zonal anatomy of the uterus. The myometrial layers
are indistinguishable on T1 imaging. It can be divided into three zones
on T2 weighted imaging7
:
• high T2 signal of endometrium
• low T2 signal of inner myometrium, known as the junctional zone
• intermediate T2 signal of the outer myometrium .
15.
Mullerian duct anomalies
Europeanclassification system :
• The table shows the European classification system ESHRE/ESGE from 2013.
• Class U0 is a normal uterus
• Class U1 is a dysmorphic shaped uterus either as a T-shaped cavum due to
abnormally thick uterine walls or as a T-shaped cavum due to an abnormal
outer contour (infantilis).
• Class U2 is the result of failure of resorption of the septum. There is an
internal indentation. The outer contour of the uterus is normal and this
differentiates the septate uterus from the bicorporeal uterus.
16.
• Class U3is a bicorporeal uterus with a left and right corpus as a result
of failure of fusion. The outer contour is abnormal with an external
cleft of the fundus. A bicorporeal septate uterus has both an external
cleft and a septum.
• Class U4 is a hemi-uterus as a result of unilateral failure of formation
of the Müllerian duct.
• Class U5 is an aplastic uterus as a result of bilateral failure of
formation of the Müllerian ducts.
• Class U6 are unclassified cases
Radiographic features
Ultrasound:
• shouldbe performed initially
• confirms any structural abnormalities of the genital tract
• sometimes cannot help to identify the type of MDA (especially on 2D imaging
alone)
• 3D coronal transvaginal imaging has a high degree of diagnostic accuracy and
ideally should be performed in the secretory phase of the menstrual cycle
21.
MRI:
• valuable non-invasivetechnique
• evaluation of the female pelvic anatomy
• accurate Müllerian duct anomaly classification
PELVIC INFLAMMATORY DISEASE
•Pelvic inflammatory disease (PID) is a broad term that encompasses a
spectrum of infection and inflammation of the upper female genital
tract, resulting in a range of abnormalities.
• PID is defined as an acute clinical syndrome associated with ascending
spread of micro-organisms, unrelated to pregnancy or surgery. The
infection generally ascends from the vagina or cervix (cervicitis) to the
endometrium (endometritis), then to the fallopian tubes (salpingitis,
hydrosalpinx, pyosalpinx), and then to and/or contiguous structures
(oophoritis, tubo-ovarian abscess, peritonitis).
25.
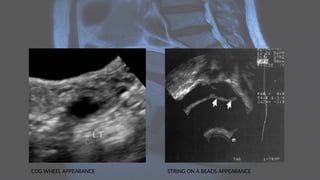
Radiographic features
Ultrasound
• Ultrasoundis usually the first imaging requested in a case of lower abdominal pain.
• Early findings in PID include :
• indistinct uterine margins
• echogenic pelvic fat
• fallopian tube thickening
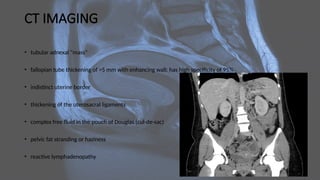
CT IMAGING
• tubularadnexal "mass"
• fallopian tube thickening of >5 mm with enhancing wall: has high specificity of 95%
• indistinct uterine border
• thickening of the uterosacral ligaments
• complex free fluid in the pouch of Douglas (cul-de-sac)
• pelvic fat stranding or haziness
• reactive lymphadenopathy
29.
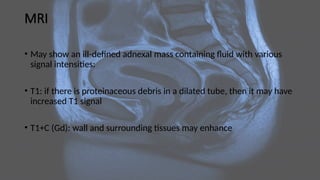
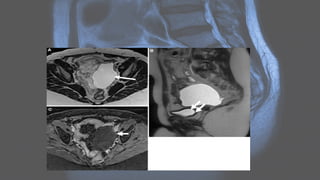
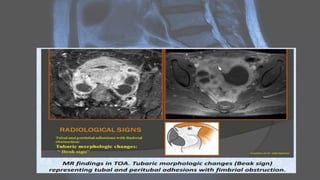
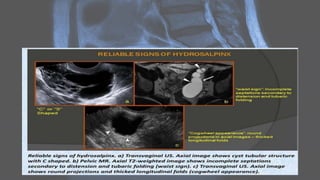
MRI
• May showan ill-defined adnexal mass containing fluid with various
signal intensities:
• T1: if there is proteinaceous debris in a dilated tube, then it may have
increased T1 signal
• T1+C (Gd): wall and surrounding tissues may enhance
33.
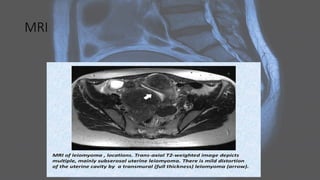
Uterine leiomyomas
• Uterineleiomyomas, also known as uterine fibroids, are benign
tumors of myometrial origin and are the most common solid benign
uterine neoplasms. They are a common incidental finding on imaging
and rarely cause diagnostic dilemma.
Plain radiograph
• Popcorn calcification within the pelvis may suggest the diagnosis.
35.
Ultrasound
• Ultrasound isused to diagnose the presence and monitor the growth of fibroids:
• uncomplicated leiomyomas are usually hypoechoic, but can be isoechoic, or even
hyperechoic compared to normal myometrium
• calcification is seen as echogenic foci with shadowing
• cystic areas of necrosis or degeneration may be seen
• Venetian blind artifact may be seen but edge shadowing +/- dense posterior
shadowing from calcification is also typically seen 17
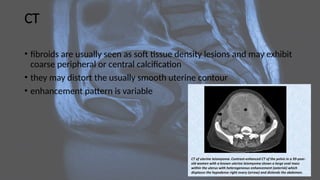
CT
• fibroids areusually seen as soft tissue density lesions and may exhibit
coarse peripheral or central calcification
• they may distort the usually smooth uterine contour
• enhancement pattern is variable
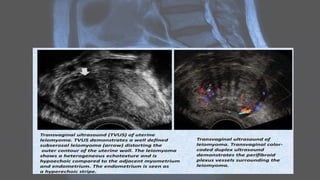
Adenomyosis
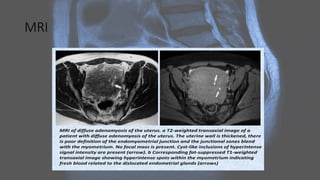
• Adenomyosis (oruterine adenomyosis) is a common uterine
condition of ectopic endometrial tissue in the myometrium,
sometimes considered a spectrum of endometriosis. Although most
commonly asymptomatic, it may present with menorrhagia and
dysmenorrhea.
• Pelvic imaging (i.e. ultrasound, MRI) may show characteristic findings,
commonly including focal or diffuse myometrial bulkiness, which may
be asymmetrical, and heterogeneous myometrium.
42.
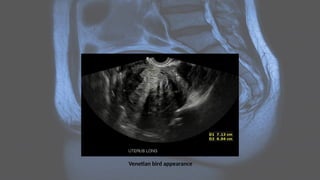
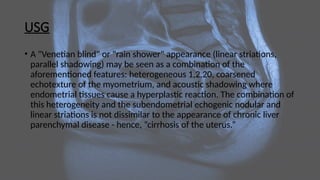
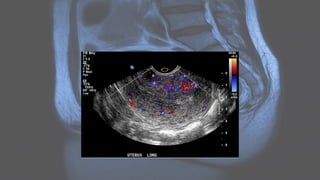
USG
• A "Venetianblind" or "rain shower" appearance (linear striations,
parallel shadowing) may be seen as a combination of the
aforementioned features: heterogeneous 1,2,20, coarsened
echotexture of the myometrium, and acoustic shadowing where
endometrial tissues cause a hyperplastic reaction. The combination of
this heterogeneity and the subendometrial echogenic nodular and
linear striations is not dissimilar to the appearance of chronic liver
parenchymal disease - hence, “cirrhosis of the uterus.”
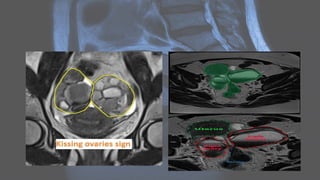
Endometriosis
• Endometriosis isa common, chronic gynecological condition defined
as the presence of functional endometrial glands and stroma-like
lesions outside the uterus. It manifests in three ways: superficial
(peritoneal) disease, ovarian disease (endometriomas), and deep
endometriosis.
• Endometriosis is highly associated with adenomyosis (in which
endometrial tissue is confined to the uterine musculature). Size
varies, ranging from microscopic endometriotic implants to large cysts
(endometriomas) and nodules. Deep infiltrating endometriosis is
complex and surgically challenging.
47.
PATHOLOGY
• metastatic theory:transplantation of endometrial cells (via retrograde
menstruation, lymphatic or vascular dissemination, iatrogenic
implantation) with probable immune/hormonal/inflammatory
mediators 8
; supporting this theory is that up to 90% of women have
bloody peritoneal fluid during the perimenstrual period 9
• metaplastic theory: retroperitoneal deep endometriosis may originate
from metaplasia of Müllerian remnants located in the rectovaginal
septum 10
• induction theory: whereby shed endometrium releases substances that
induce undifferentiated mesenchyme to form endometriotic tissue 2