Downloaded 30 times


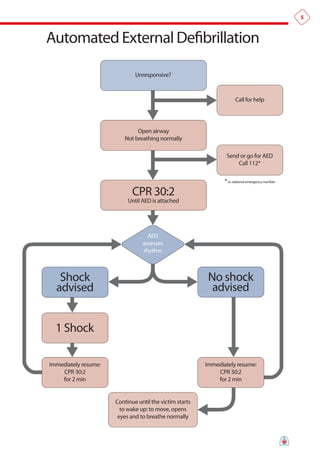

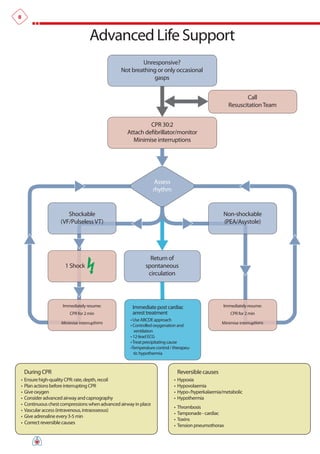










The document summarizes the main changes in resuscitation guidelines from 2010 compared to 2005. Key changes include an increased focus on high-quality chest compressions with minimal interruptions, continuing compressions when charging a defibrillator to reduce delays, and removing recommendations for a specified period of CPR before defibrillation for unwitnessed arrests. The guidelines emphasize the importance of early defibrillation and avoiding long pause times both before and after shocks.

![Poster 10 als_01_01_eng_v20100927[1]](https://cdn.slidesharecdn.com/ss_thumbnails/poster10als0101engv201009271-120904135505-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)











![All posters gl2010_english[1]](https://cdn.slidesharecdn.com/ss_thumbnails/allpostersgl2010english1-120830095239-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























































