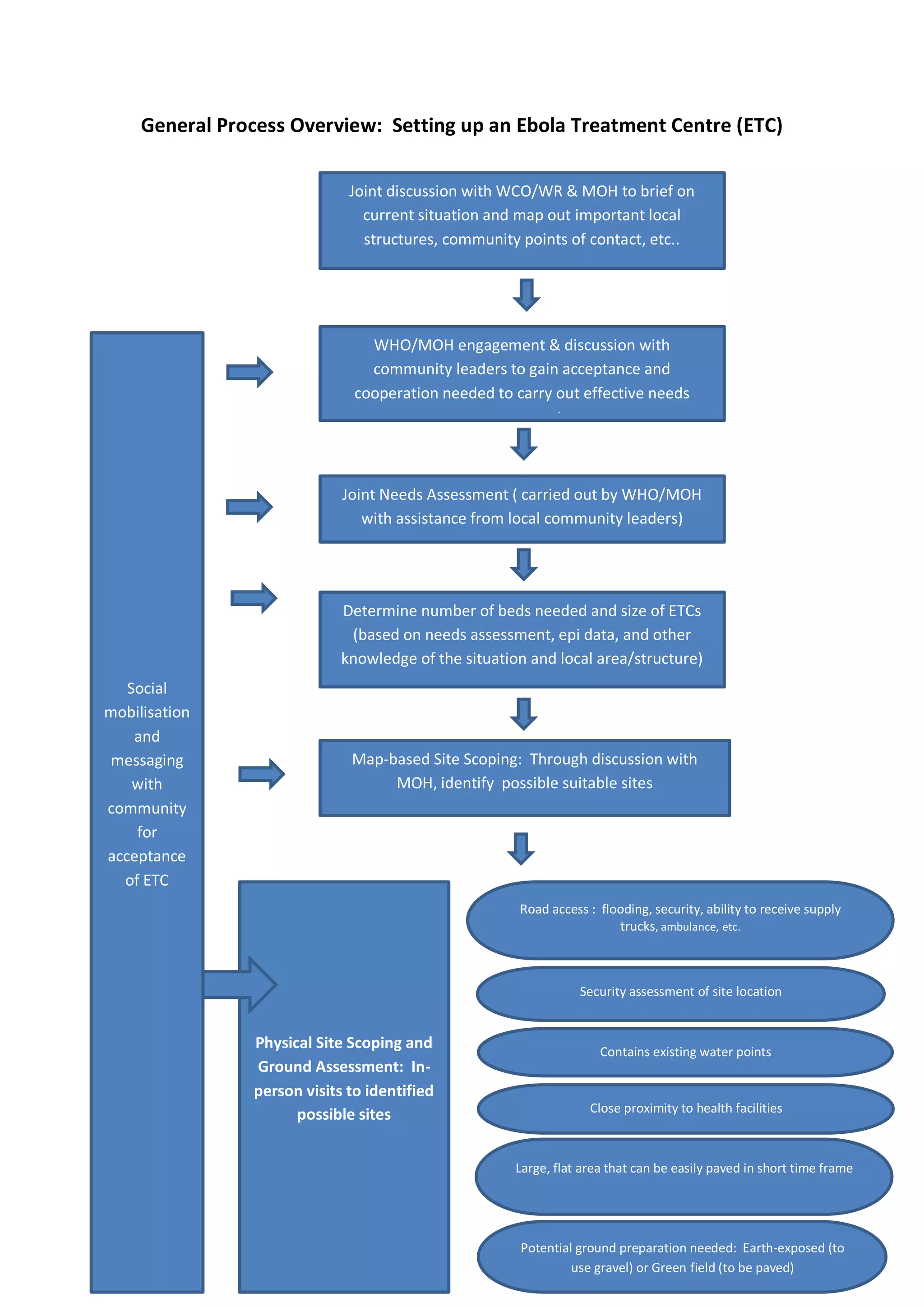
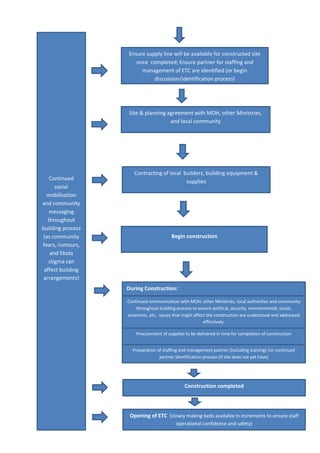
Setting up an Ebola Treatment Centre (ETC) requires careful planning and design to mitigate the risk of infection. Key requirements include:
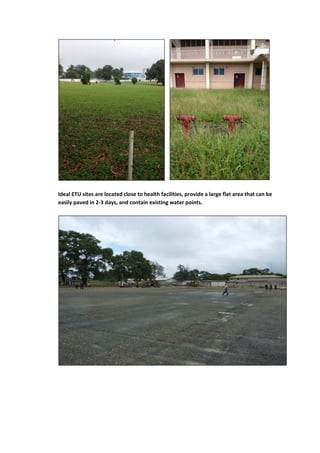
1) Locating the ETC near existing health facilities for easier patient triage and laboratory access.
2) Designing separate areas for suspect and confirmed patients, with strict controls on staff and patient flow to prevent cross-contamination.
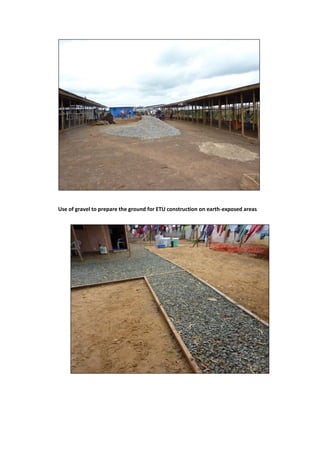
3) Ensuring adequate water, sanitation and waste management facilities as well as personal protective equipment for staff.
4) Establishing a Rapid Response Team of medical staff to oversee operations and ensure all services meet safety standards for both staff and patients.






























![[TMMC Healthcare] Ebola prevention procedure](https://cdn.slidesharecdn.com/ss_thumbnails/ebolaprocedure-en-141120212922-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)



























