Estimating the Costs of Public Sector Provision of the Bangladesh Essential Health Service Package (2016 – 2022) - Part 1
•
0 likes•130 views

Estimating the Costs of Public Sector Provision of the Bangladesh Essential Health Service Package (2016 – 2022) - Part 1

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Estimating the Costs of Public Sector Provision of the Bangladesh Essential Health Service Package (2016 – 2022) - Part 1
Similar to Estimating the Costs of Public Sector Provision of the Bangladesh Essential Health Service Package (2016 – 2022) - Part 1 (20)
More from HFG Project
More from HFG Project (20)
Recently uploaded
Recently uploaded (20)
Estimating the Costs of Public Sector Provision of the Bangladesh Essential Health Service Package (2016 – 2022) - Part 1
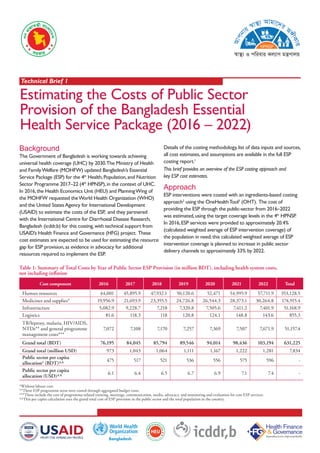
- 1. Estimating the Costs of Public Sector Provision of the Bangladesh Essential Health Service Package (2016 – 2022) Background The Government of Bangladesh is working towards achieving universal health coverage (UHC) by 2030.The Ministry of Health and FamilyWelfare (MOHFW) updated Bangladesh’s Essential Service Package (ESP) for the 4th Health,Population,and Nutrition Sector Programme 2017–22 (4th HPNSP),in the context of UHC. In 2016,the Health Economics Unit (HEU) and PlanningWing of the MOHFW requested theWorld Health Organization (WHO) and the United StatesAgency for International Development (USAID) to estimate the costs of the ESP, and they partnered with the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) for this costing,with technical support from USAID’s Health Finance and Governance (HFG) project. These cost estimates are expected to be used for estimating the resource gap for ESP provision,as evidence in advocacy for additional resources required to implement the ESP. Details of the costing methodology,list of data inputs and sources, all cost estimates,and assumptions are available in the full ESP costing report.1 Approach ESP interventions were costed with an ingredients-based costing approach2 using the OneHealthTool3 (OHT). The cost of providing the ESP through the public-sector from 2016–2022 was estimated,using the target coverage levels in the 4th HPNSP. In 2016,ESP services were provided to approximately 20.4% (calculated weighted average of ESP intervention coverage) of the population in need;this calculated weighted average of ESP intervention coverage is planned to increase in public sector delivery channels to approximately 33% by 2022. This brief provides an overview of the ESP costing approach and key ESP cost estimates. Cost component 2016 2017 2018 2019 2020 2021 2022 Total Human resources 44,001 45,895.9 47,932.1 50,120.6 52,471 54,995.9 57,711.9 353,128.5 Medicines and supplies* 19,956.9 21,693.9 23,355.5 24,726.8 26,544.3 28,373.1 30,264.8 174,915.4 Infrastructure 5,082.9 9,228.7 7,218 7,320.8 7,505.6 7,411.2 7,401.9 51,168.9 Logistics 81.6 118.3 118 120.8 124.1 148.8 143.6 855.3 TB/leprosy, malaria, HIV/AIDS, NTDs** and general programme management costs*** 7,072 7,108 7,170 7,257 7,369 7,507 7,671.9 51,157.4 Grand total (BDT) 76,195 84,045 85,794 89,546 94,014 98,436 103,194 631,225 Grand total (million USD) 973 1,043 1,064 1,111 1,167 1,222 1,281 7,834 Public sector per capita allocation4 (BDT)^^ 475 517 521 536 556 575 596 - Public sector per capita allocation (USD)^^ 6.1 6.4 6.5 6.7 6.9 7.1 7.4 - *Without labour cost. **These ESP programme areas were costed through aggregated budget costs. ***These include the cost of programme-related training, meetings, communication, media, advocacy, and monitoring and evaluation for core ESP services. ^^This per capita calculation uses the grand total cost of ESP provision in the public sector and the total population in the country. Table 1: Summary of Total Costs by Year of Public Sector ESP Provision (in million BDT), including health system costs, not including inflation Technical Brief 1 Bangladesh
- 2. DISCLAIMER Suggested Citation: Ministry of Health and FamilyWelfare. June 2018.Technical Brief 1. Estimating the Costs of Public Sector Provision of the Bangladesh Essential Health Service Package: 2016-2022. Dhaka: Ministry of Health and FamilyWelfare, Government of the People’s Republic of Bangladesh. The cost estimation was done for the ten public sector delivery channels for the ESP in urban and rural areas, covering the six core ESP service areas:maternal,neonatal, child & adolescent health (MNCAH),family planning,nutrition, communicable diseases,non-communicable diseases (NCD), and management of other common conditions.The icddr,b study team consulted with a range of stakeholders,partners, the National OHT Resource Pool,international OHT experts, and expert reviewers from HFG andWHO to estimate the costs of the ESP. documents,5 and interviews at selected sites.Intervention costs were estimated using data from a mixture of 2016 practices,standard protocols (where available),and expert opinions. With this data,the cost per case per year of each intervention was estimated,using the medicines and supplies required to deliver the particular intervention and a cost per minute of medical personnel time required to provide the intervention.The study team also calculated a weighted average cost per service for each intervention,as the cost per service per person varied by delivery channel. ESP Cost Estimates The total cost of delivering the ESP in 2016 was BDT 76,195 million (USD 973 million),based on the actual coverage data and assumptions for that year (Table 1);this total cost million (USD 1,281 million) in 2022 taking into account the cost of current and new services,assumptions,and reaching the targets per year in the operational plans of the 4th HNPSP (2017–2022).In the base year (2016),human resources accounted for the highest proportion of the total cost (58%), followed by drugs and supplies (26%). With respect to the six core ESP services,MNCAH accounted for approximately 57% of total costs in 2016,and is estimated to decrease to 44% by 2022.Concurrently NCD costs are expected to increase from 19% to 31% due to planned expansion of NCD services as part of the 4th HPNSP. 6 in 2016 was BDT 2,349 (USD 29.8);this gradually decreases to BDT 1,805 (USD not include health system costs. Recommendations Comprehensive provision of the ESP in Bangladesh is a critical part of the government’s efforts towards achieving UHC. These cost estimates will support the MOHFW and others services during the period 2017–22. These results provide an estimate of the annual implement for public sector provision of the ESP. Policy planners may consider these estimates and use them to advocate for increased funding for health. The National OHT Resource Pool should work under an institutional framework of the MOHFW to conduct additional costing exercises, including using standard treatment protocols for all services; these scenarios will be useful for the mid-term review of the 4th HPNSP and for planning of the next sector program. Ingredients- based costing of TB, malaria, HIV/AIDS and Neglected tropical diseases (NTDs) interventions should be undertaken. As the country moves towards UHC by 2030, future analyses should look at the cost of full coverage of ESP services. Future ESP cost estimates should also use standard protocols (normative costs) for all guidelines are not available, to identify the gap between current practice and protocols, and to provide planners with evidence to advocate for increase funding for the provision of quality ESP services across all relevant delivery channels. Figure 1: Average Cost of the ESP Provision per Beneficiary, in USD, 2016–2022 1 Health Economics Unit, Ministry of Health and Family Welfare and World Health Organization, Bangldesh, ‘Costs of the Bangladesh Essential Health Service Package: 2016–2022’ March 2018. 2 Due to time and budget constraints, the cost of TB, HIV/AIDS, malaria, and NTD programmes were estimated using aggregate programme costs obtained from key implementing partners. 3 The OHT is designed to support medium- to long-term (3 to 10 years) strategic planning in the health sector, and has been used to inform strategic planning processes in more than 30 low- and middle-income countries to date. 4 OHT calculates cost per capita by dividing the total cost calculated for ESP provision by the total population in a given year. 5 Health Bulletin, Bangladesh Demographic Health Survey reports and dataset, morbidity survey, urban health survey, literature search, and family planning management information system. 6 The cost per beneficiary does not include inflation but does include both health service and health system costs. It only applies to those ESP interventions for which costs were estimated at a specific coverage, and does not represent a single client, who would typically need a mix of services. 29.8 27.7 26.3 25.0 24.0 23.1 22.4 0 5 10 15 20 25 30 35 40 2016 2017 2018 2019 2020 2021 2022 USD Year