Downloaded 86 times

























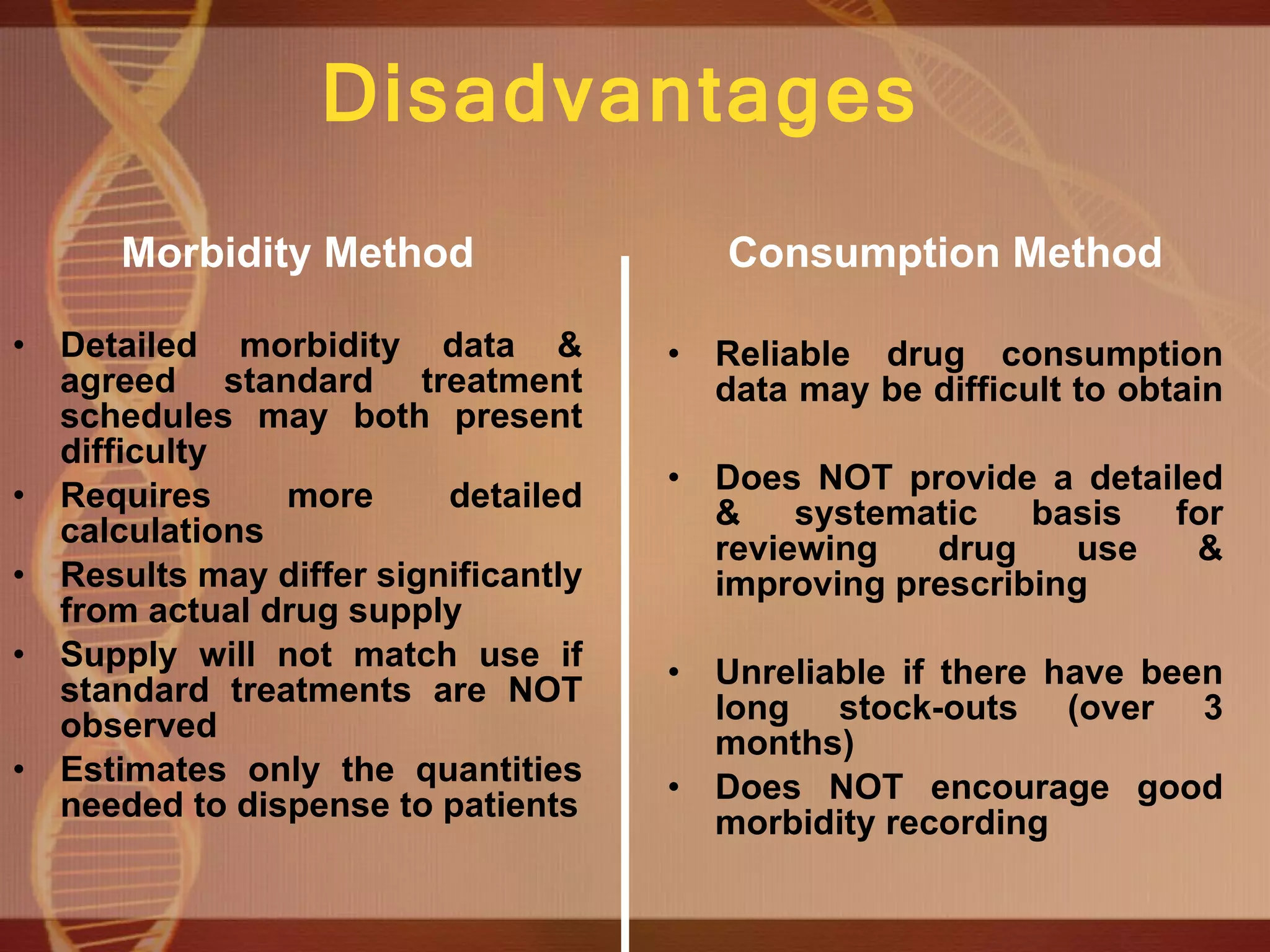











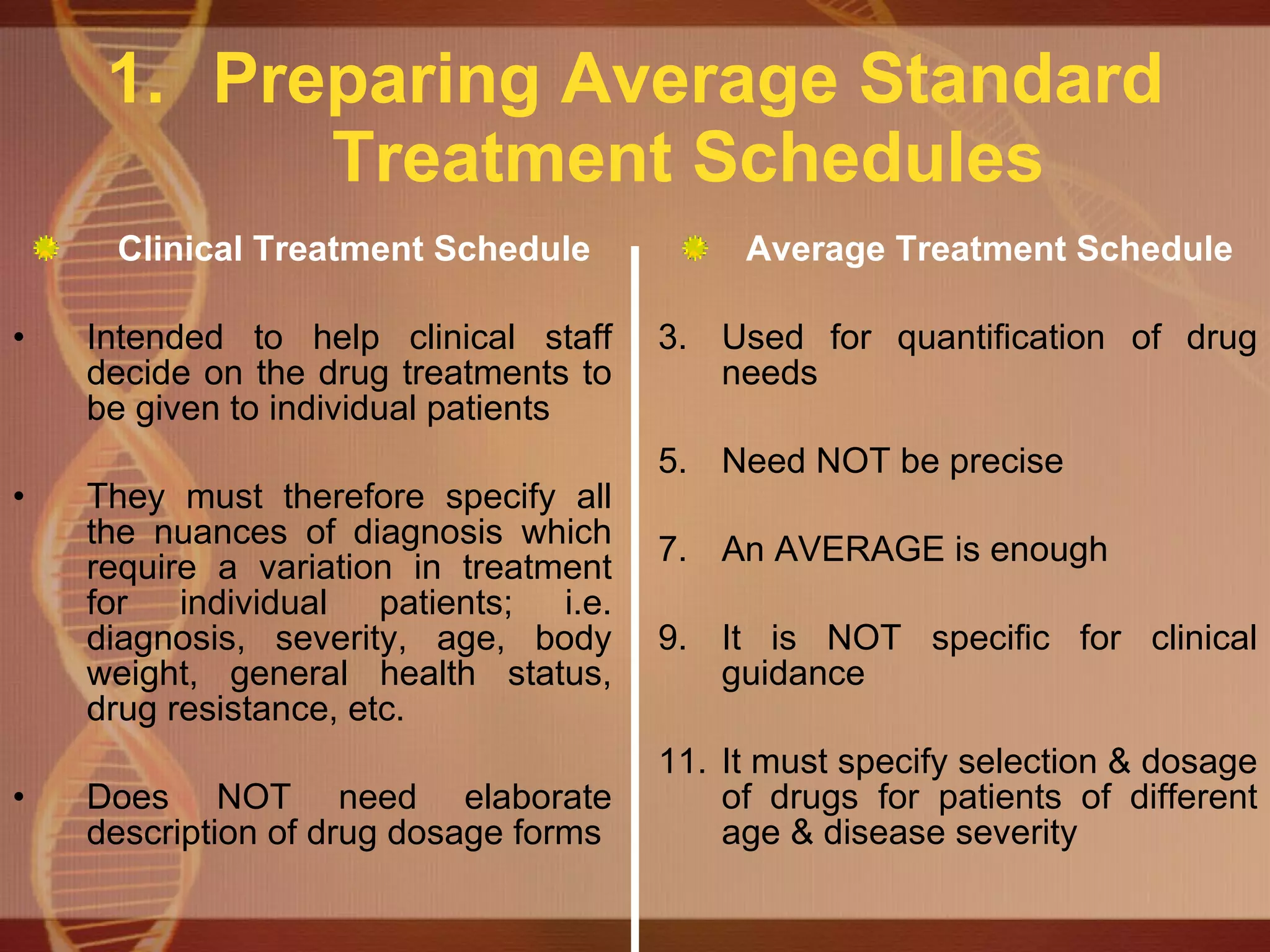






















This document discusses effective drug supply management through quantification, which is estimating how much of each drug is needed. It describes the components of an effective system including selection, quantification, procurement, distribution, and use. Poor quantification can be seen through chronic shortages and surpluses, inequity between facilities, inadequate cost-effectiveness, irrational adjustments, and suppressed demand. The two main quantification methods described are the morbidity method based on standard treatments and episodes, and the consumption method based on past usage.