This lecture can serve as a bullet-point review of the emergency studies in nuclear medicine. The outline is as follows:
- Pulmonary Embolism.
- GI Bleeding.
- ATN.
- Shunt Patency.
- Brain Death.
Outlines :
1. VQscan in PE.
2. GI Bleeding Studies.
3. ATN in Renogram.
4. Shunt patency study .
5. Brain Perfusion scan.
3.
VQ scan inPE.
• Pulmonary embolism is a treatable disease caused by thrombus
formation in the lung vasculature.
• The diagnosis of pulmonary embolism is based on imaging.
• CTPA and ventilation-perfusion (V/Q) scan are the two most common
and widely used modalities to diagnose PE.
V/Q SPECT ImagingTechnique
• (SPECT) obtains the image through multidetector gamma-cameras to
generate 3-dimensional images.
• SPECT has higher sensitivity than the planar technique.
• If the CTPA contrast and radiation exposure are contraindicated or
must be avoided, the V/Q SPECT is considered the second-line
diagnostic test
6.
Advantages of theV/Q SPECT :
1. Low indetermination rate.
2. Greater sensitivity ( 97% ) and specificity (91%) .
7.
V/Q Planar ImagingTechnique
• Planar imaging acquisition is a 2D technique obtained through a dual-
head gamma camera for ventilation and perfusion .
• Limited patient movement between the 2 scans is crucial.
• This technique is used with at least 4 views when the V/Q SPECT is
not performed .
8.
Disadvantages of planarV/Q :
1. Inaccurate determination of segment involvement .
2. Difficult to determine the degree of perfusion defects.
Interpretation by which Criteria ?
9.
V/Q SPECT/CT
• Thistechnique integrates a low-dose CT scan with SPECT to provide
more detailed anatomic information.
• The CT usually done without contrast, after the perfusion scan.
• Radiation exposure is the main disadvantage.
10.
Advantages of SPECT/CT:
1.More accurate in the detection of other mismatch defects that are
not PE, such as in obstructive lung disease, external vascular
compression, or neoplasm.
2. Better anatomical information (pneumonia, pleural, or pericardial
effusion).
3. Detection of pulmonary embolism cases in which V/Q is unusually
matched, like PE, with an area of pulmonary infarction.
4. Has the highest diagnostic accuracy compered to SPECT and Planar .
11.
Indications of VQscan:
• VQ scan mainly preserved for a patients in whom CTPA is
contraindicated (pregnancy, renal insufficiency, chronic kidney
disease, or severe contrast allergy) .
V/Q is the test of choice in pregnant females with suspected
pulmonary embolism .Why?
12.
Interpretations
• The Interpretationdepends on the protocol that you are following in
your institute .
• If it Planar VQ scan , use Modified PIOPED II criteria or Perfusion-only
PISAPED criteria.
13.
Perfusion-only PISAPED criteria
1.PISAPED stands for the prospective investigative study of acute pulmonary embolism diagnosis.
2. It is simple and eliminates nondiagnostic readings.
3. Combines only the perfusion part of the V/Q scan with CXR.
4. PISAPED criteria are classified based on the following scan findings:
PE Present:
One or more wedge-shaped perfusion defects.
PE Absent:
1. No perfusion defects.
2. Non-wedge-shaped perfusion defect.
3. Non segmental defects caused by the mediastinum, diaphragm, or an enlarged heart.
14.
SPECT and SPECTCT criteria
EANM guideline for ventilation/perfusion single-photon emission computed tomography (SPECT) for diagnosis of pulmonary embolism and beyond
15.
GI Bleeding Studies.
1.Divided to upper and lower GI bleeding based on the location
(ligament of Treitz).
2. Mainly used to Identify the level of lower GI bleeding to assist
angiographic or surgical intervention.
3. For upper GI bleeding, typically NG aspiration and endoscopy are
used for diagnosis. No role of Nuclear GI bleeding studies.
Interpretations
1. Focal siteof increased activity.
2. Conforms to bowel anatomy.
3. Increases with time.
4. Moves antegrade or sometimes retrograde in bowel.
• Sensitivity and specificity :
91% sensitivity and 95% specificity
ATN in Renogram
1.ATN Occurs in 25-40% of tranplants (mostly cadaveric).
2. Usually in the post-op period with spontaneous resolution.
3. Self limiting, usually resolved within 2 weeks.
20.
Interpretations:
Flow is preservedbut transit time is increased and there is
parenchymal retention.
Renal Scintigraphy in the Acute Care Setting
22.
Shunt patency study
1.Variety of CSF shunts are avalible (ventriculoperitoneal,
ventriculoatrial, ventriculopleural, lumboperitoneal) have been
used to treat hydrocephalus.
2. Complications may affect the drainage ,include catheter blockage,
infection, thromboembolism, subdural or epidural hematomas,
disconnection of catheters, CSF pseudocyst, bowel obstruction, and
bowel perforation.
23.
• The diagnosisof shunt patency and adequacy of CSF flow often can
be made by examination of the patient and inspection of the
subcutaneous CSF reservoir.
• When this assessment is uncertain, radionuclide studies with In-111
DTPA or Tc-99m DTPA are useful for confirming the diagnosis.
• Familiarity with the specific shunt type and its configuration is helpful.
For example, the valves may allow bidirectional or only unidirectional
flow ( IMPORTANT).
25.
• Patency ofthe proximal shunt limb can sometimes be evaluated
before checking distal patency.
• In patients with certain types of variable or low-pressure two-way
valves, the distal catheter is initially occluded by manually pressing on
the neck. The pressure may cause injected tracer to flow into the
proximal limb. Images should show prompt flow into the ventricles,
followed by spontaneous distal flow through the shunt catheter .
26.
• Resistance atthe time of injection always indicates malfunction of
the shunt.
• If there is proximal limb malfunction, either no activity will reflux into
the ventricle and there will be rapid transit of the
radiopharmaceutical through the distal shunt into the peritoneal
cavity.
29.
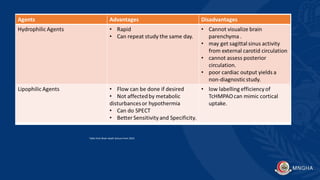
Brain Death
• Tracers:
1. Hydrophilic agents (Tc-glucoheptonate, Tc-DTPA, TcO4) .
2. Lipophilic agents (Tc 99 m HMPAO).