Download as PDF, PPTX

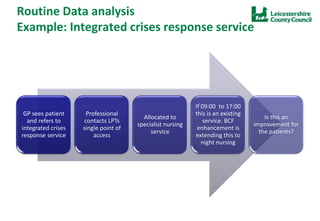

The document evaluates Leicestershire’s Better Care Fund programme, focusing on integrating health and care services through a pooled budget and enhanced community capacity. Key objectives include reducing permanent admissions, improving patient experiences, and analyzing outcomes through data linkage and clinical audits. Future steps involve procurement for evaluations, ongoing research collaborations, and proposals for further cohort analysis.






















































































