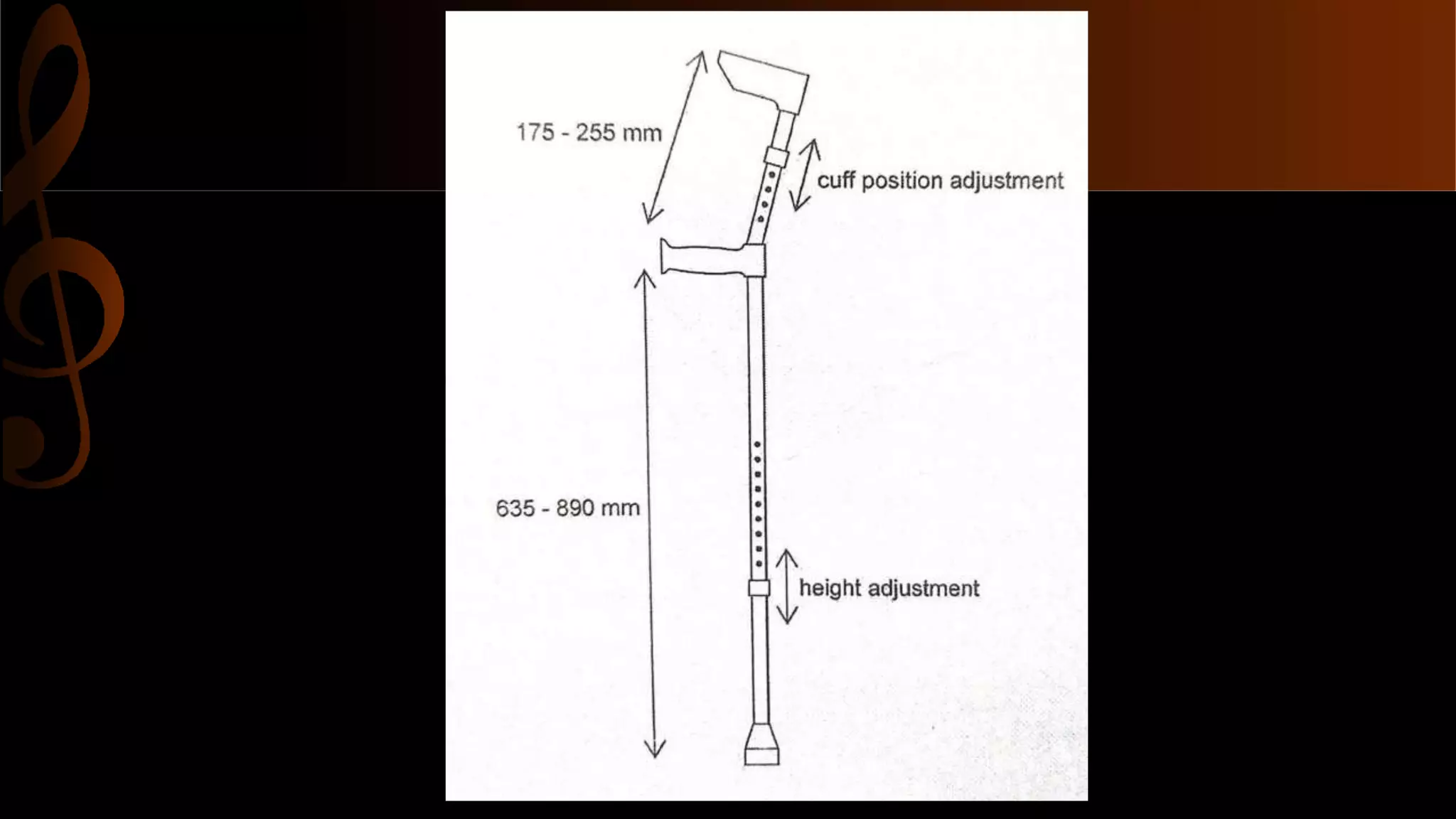
This document discusses elbow crutches. It defines elbow crutches as forearm crutches that have a cuff that supports the user's forearm. The crutches are made of aluminum and adjust in length and cuff position. They transfer 40-50% of body weight and are suitable for patients with good balance and strong arms. The advantages are that the forearm cuff allows hand use and functional stair climbing, while disadvantages include less lateral support and difficulty removing cuffs. The cuff should be placed at the proximal third of the forearm.