Downloaded 67 times
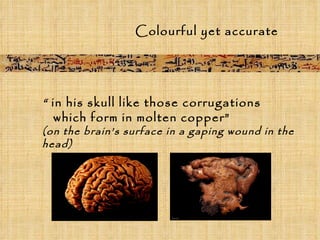
![Case 2 Title : Instructions concerning a [gaping] wound [in his head], penetrating to the bone. Examination : If thou examinest a man having a [gaping] wound [in] his [head], penetrating to the bone, thou shouldst pal[pate hi]s [wound]. If thou findest his skull [uninjured, not hav]ing a perforation in it... Instructions concerning a [gaping] wound [in his head], penetrating to the bone.](https://image.slidesharecdn.com/edwinsmithpapyrus1sttexbookinsurgery07-111107115833-phpapp02/85/Edwin-smith-papyrus-1st-texbook-in-surgery-07-15-320.jpg)
![Case 2 Diagnosis : Thou shouldst say regarding [him]: "One hav[ing a gaping wou]nd in his head. An ailment which I will treat.“ Treatment : [Thou] shouldst bind [fresh meat upon it the first day; thou shouldst apply for him two strips of linen, and treat afterward with grease, honey, (and) lin]t every day until he recovers. Gloss : As for: "Two strips of linen," [it means] two bands [of linen which one applies upon the two lips of the gaping wound in order to cause that one join] to the other.](https://image.slidesharecdn.com/edwinsmithpapyrus1sttexbookinsurgery07-111107115833-phpapp02/85/Edwin-smith-papyrus-1st-texbook-in-surgery-07-16-320.jpg)
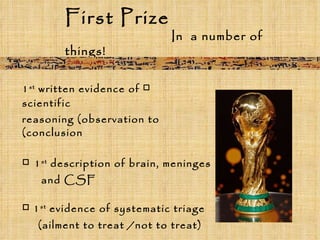
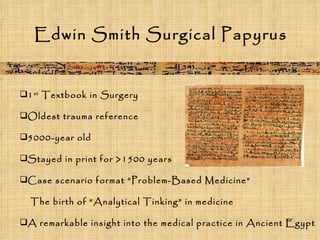

The Edwin Smith Papyrus, dating back to around 1700 BC, is recognized as the first textbook in surgery, providing significant insights into ancient Egyptian medical practices. It describes 48 surgical cases with diagnostic methods and treatment instructions, marking a pivotal development in analytical thinking in medicine. This ancient treatise remained in circulation for over 1500 years and showcases advanced medical knowledge for its time.


























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








