Downloaded 219 times
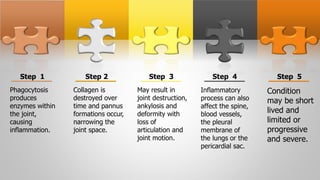
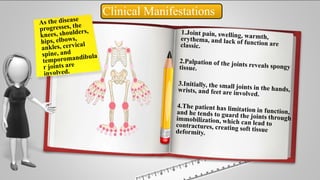
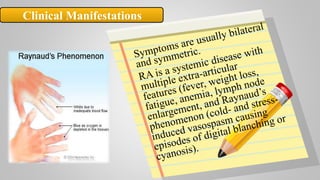
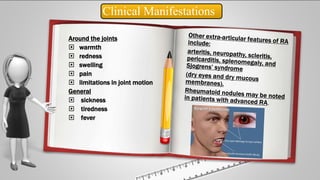




Rheumatoid arthritis is a chronic autoimmune disease that causes inflammation of the joints. It affects around 1% of the adult population globally. The disease is characterized by destruction and proliferation of the synovial membrane that lines the joints, causing pain, swelling, stiffness and limited range of motion. Diagnosis involves assessing symptoms, laboratory tests showing inflammation, and x-rays that can reveal bone erosion over time. Treatment aims to reduce inflammation, slow joint damage, and improve function through medications, exercise, joint protection, and nutritional support. Nursing care focuses on pain management, maintaining mobility and independence with daily activities.