Downloaded 68 times
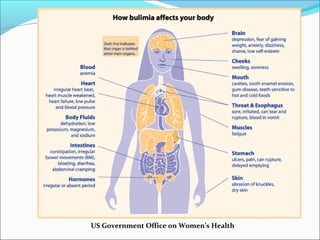
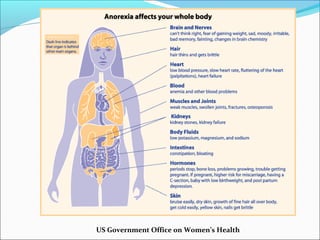




This document outlines information about eating disorders including definitions, health consequences, risk factors, prevalence, prevention, and treatment. It defines eating disorders as conditions characterized by abnormal eating habits caused by biological, psychological, and environmental influences. The document discusses specific eating disorders like anorexia nervosa, bulimia nervosa, and binge eating disorder. It also provides statistics on the prevalence of eating disorders in the United States and risk factors. The document concludes by discussing evidence-based approaches to prevention and treatment of eating disorders.