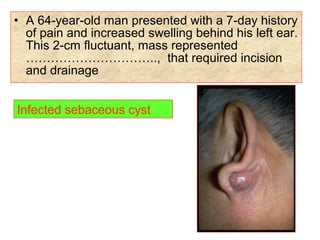
Downloaded 80 times
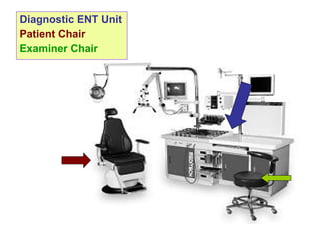
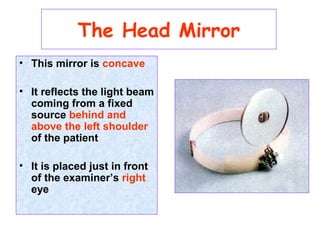
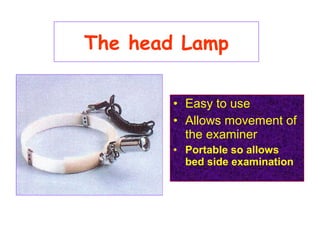
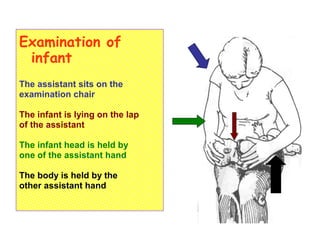
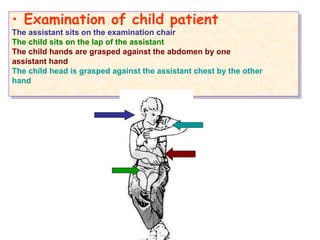
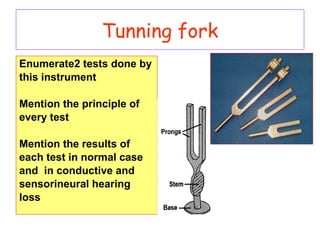

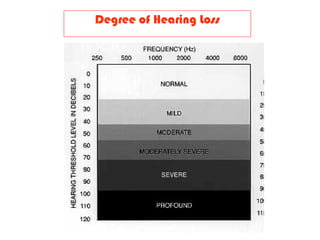
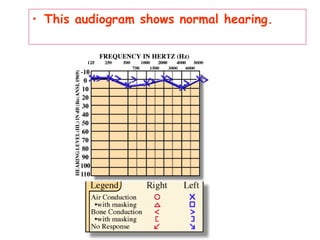
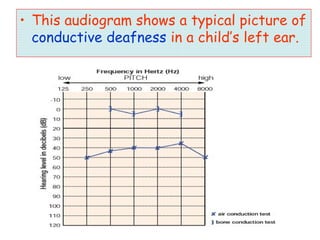
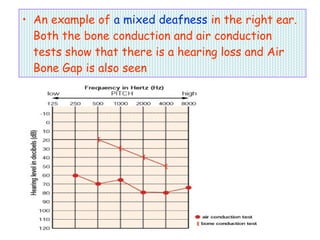
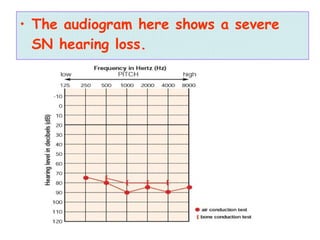
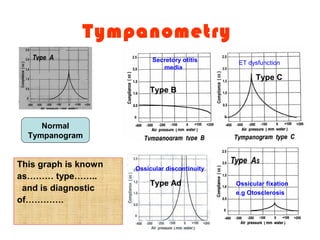
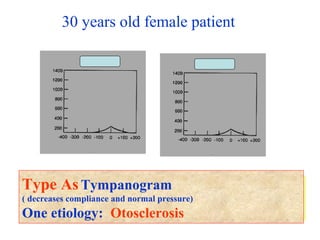
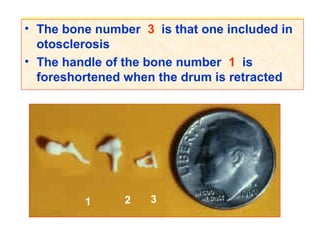
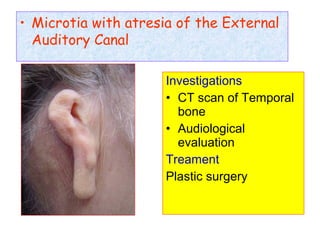
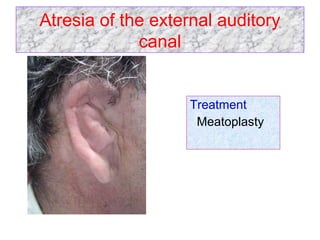
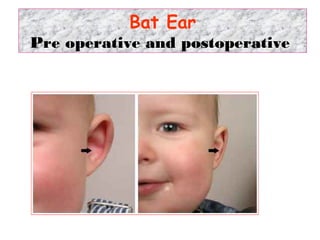

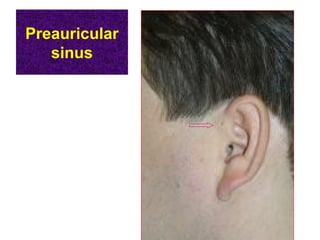
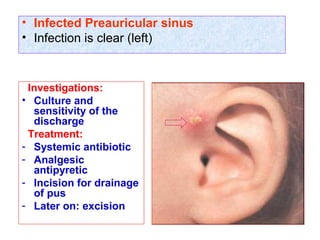
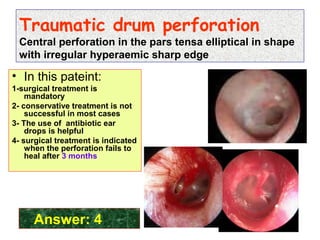
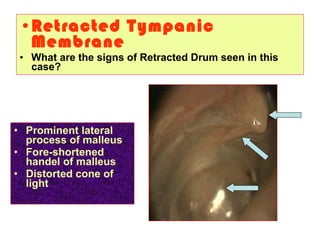
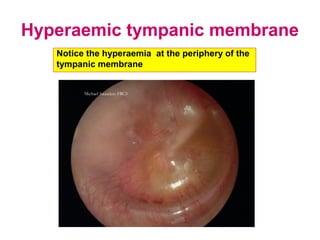




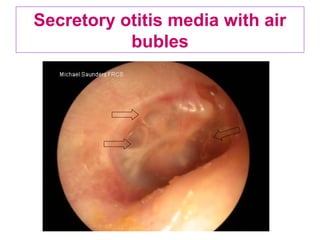
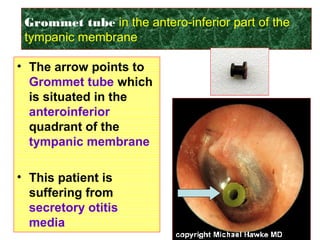

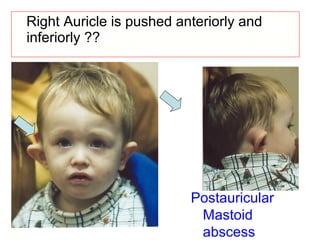
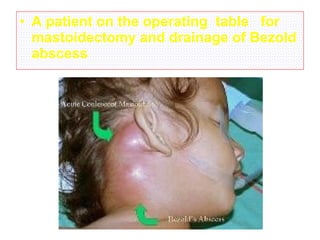
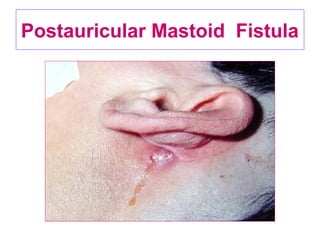
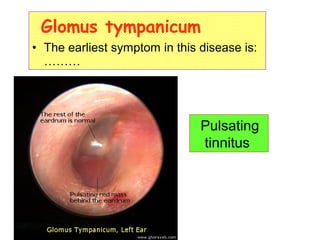



The document describes various equipment, techniques, and procedures used in otolaryngologic examinations. It includes descriptions of: - Examination chairs and mirrors used to examine patients' ears, nose, and throat - Techniques for examining infants and children with an assistant's help - Common tests performed including tuning fork tests, audiometry, and tympanometry - Otoscopic examination techniques using different specula and equipment - Examination of the ear drum and conditions that affect its appearance - Surgical and non-surgical treatment options for various ear conditions