This document discusses fluid and electrolyte disorders, focusing on sodium, potassium, and water regulation. It covers:
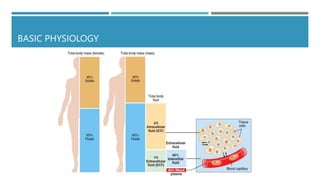
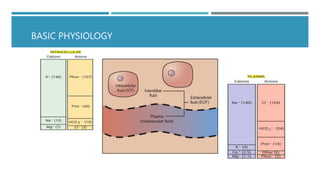
1) The roles of sodium, potassium, and water in the body and their regulation primarily by the kidney.
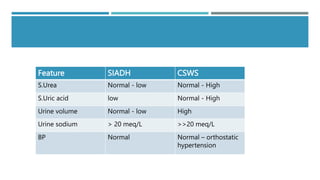
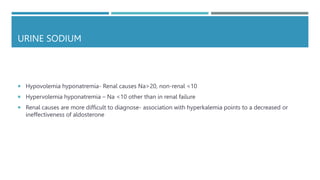
2) Common disorders of sodium and potassium balance like hyponatremia, hypernatremia, and hyperkalemia.
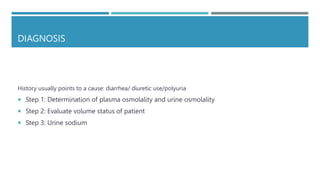
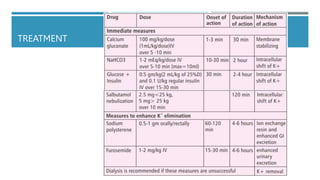
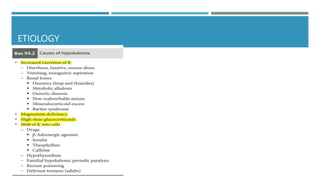
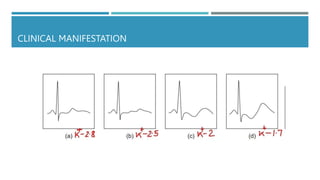
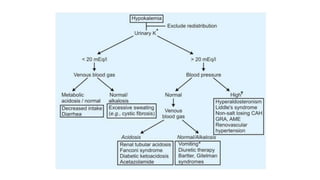
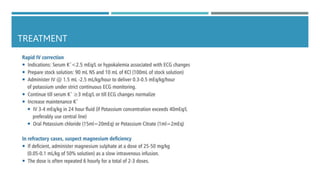
3) The evaluation, causes, clinical manifestations, and treatment approaches for various electrolyte imbalances based on case examples provided.