Downloaded 282 times
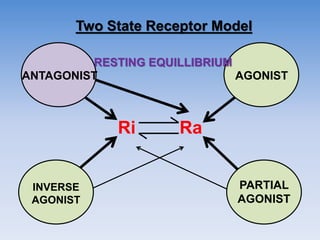
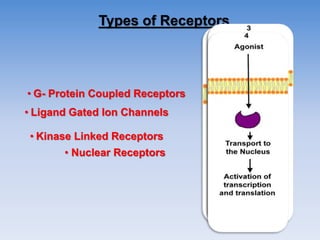
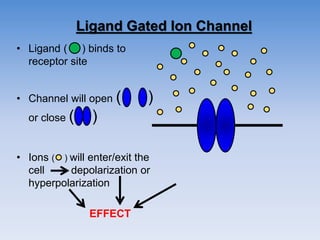
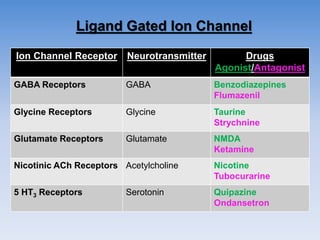
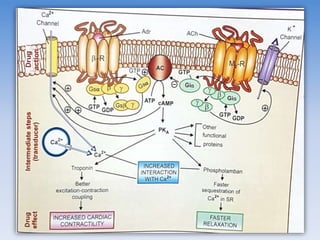
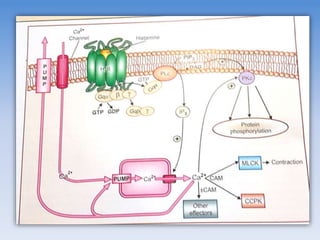
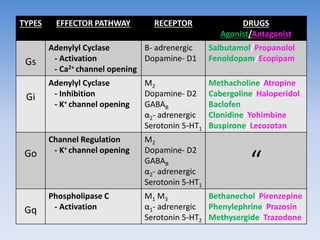
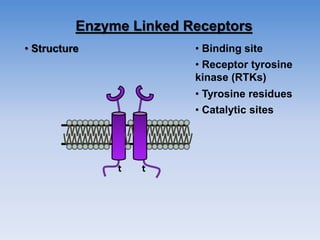


The document outlines key concepts related to drug-receptor interactions, including definitions, historical theories, and types of receptors. It discusses mechanisms such as receptor activation, pharmacological effects, receptor regulation, and the role of various ligands. Additionally, it covers specific receptor types including ligand-gated ion channels, G-protein coupled receptors, and enzyme-linked receptors, along with implications in pharmacology and associated diseases.




























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)












