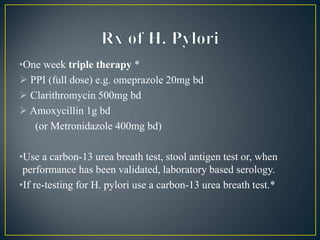
This document discusses functional dyspepsia, also known as indigestion. It is characterized by chronic or recurrent pain in the upper abdomen and feeling full earlier than expected when eating. Approximately 50% of patients have motor disorders in the stomach and small bowel. Treatment options include lifestyle changes, antacids, testing and treating for H. pylori infection, and prescribing proton pump inhibitors. Endoscopy is only recommended for those with alarm symptoms like bleeding, weight loss, or difficulty swallowing.


![• Review medications for possible causes of dyspepsia
(calcium antagonists, nitrates, theophyllines,
bisphosphonates, corticosteroids and non-steroidal
anti-inflammatory drugs [NSAIDs]).
• In patients requiring referral, suspend NSAID use.](https://image.slidesharecdn.com/copyofcopyofchapter92druginducedgitdiseasesdyspepsia-231129063938-04a037a2/85/Drug-induced-GIT-diseases-dyspepsia-ppt-9-320.jpg)