INTRODUCTION
• Donor lymphocyteinfusion (DLI) is an important treatment modality
in the management of relapsed hematological malignancies after
allogeneic hematopoietic cell transplantation (allo-HCT).
• Donor T lymphocytes can be used in a therapeutic, pre-emptive or
prophylactic manner in an attempt to stimulate a graft versus
leukemia (GVL) effect and eradicate residual disease or even prevent
relapse in a high-risk setting.
3.
DONOR LYMPHOCYTE INFUSION
•IV administration of WBC fraction of cells obtained from a donor who previously or
concurrently donated stem cells to a particular recipient.
• Most successful form of adoptive immunotherapy used after HSCT.
• Mechanism - by the graft-versus-tumor effect (GVT) or graft versus leukemia effect
(GvL).
GOALS
• Major strategy for managing relapsed bone marrow transplant patients.
• To induce a remission in the patient's cancer by destroying any residual disease
• To treat mixed chimerism (to establish full donor chimerism )
• Restore GvL effect in patients
4.
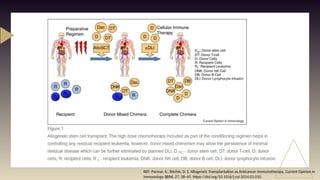
REF: Parmar, S.;Ritchie, D. S. Allogeneic Transplantation as Anticancer Immunotherapy. Current Opinion in
Immunology 2014, 27, 38–45. https://doi.org/10.1016/j.coi.2014.01.010.
5.
MECHANISM OF DLI
•DLI is primarily mediated by immune effector cells, including CD4+ T
cells, CD8+ T cells, regulatory T cells (T regs), natural killer (NK) cells,
and antigen presenting cells.
• DLI is thought to mediate GVT primarily via reversal of T cell exhaustion
in resident CD8+ T cells (a state of reduced effector function and
proliferation by T cells associated with chronic antigen exposure).
• DLI is also associated with normalization of the T cell receptor repertoire
and clonal expansion of allogeneic T cells and improved coordination of
T and B cell immunity
6.
• Process ofdonor immune cell-induced elimination of residual leukemic burden
following allogeneic HCT
• Infusion of donor hematopoietic stem cells along with allogeneic lymphoid
populations after immunosuppressive and tumor-controlling conditioning
chemotherapy results in reconstitution of hematopoiesis, expansion of lymphoid
effectors, recognition of minor histocompatibility antigens on tumor targets and
eradication of residual malignancy.
• Attributable to cytotoxic T lymphocytes (CTL) derived from mature donor derived
CD8+ T lymphocyte
GRAFT VERSUS LEUKEMIA (GvL) EFFECT
7.
REF: Parmar, S.;Ritchie, D.
S. Allogeneic
Transplantation as
Anticancer Immunotherapy.
Current Opinion in
Immunology 2014, 27, 38–
45.
https://doi.org/10.1016/j.c
oi.2014.01.010.
8.
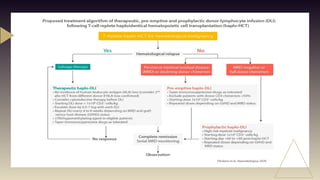
DLI may begiven:
• To treat overt disease recurrence or progression after allogeneic cell transplantation.
• As pre emptive therapy in
‐ minimal residual disease or high-risk disease.
• To promote further donor engraftment in recipients with mixed donor chimerism.
• As treatment of uncontrolled post transplant viral infections
‐ .
• As treatment for a post transplant lymphoproliferative disorder
‐ .
Rationale for donor lymphocyte infusions
REF: David C. Halverson and Daniel Fowler Experimental Transplantation and Immunology
Branch, National Cancer Institute, National Institutes of Health, Bethesda, MD, USA
9.
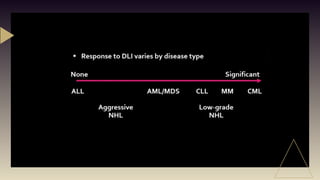
• Graft versustumor (GvT) susceptibility:
‐ ‐
CML>low grade NHL>high grade NHL>HD>MM>AML>ALL
• Transplant recipient GvHD status:
- Patients with active acute or chronic GvHD requiring ongoing immunosuppression have been
considered inappropriate candidates for DLI.
- Patients with a history of past severe GvHD must be considered high risk for GvHD recurrence
after DLI and may warrant immunosuppression concurrent to DLI.
• Primary disease status:
- DLIs are more likely to be successful in eradicating minimal amounts of disease.
- To this end, DLIs may be more effective after cytoreductive therapies.
Factors in deciding DLI
11.
• The lymphocytesused as a DLI may be either newly acquired from the donor by additional
lymphapheresis or can be in an aliquot of mobilized peripheral blood hematopoietic progenitor cells
(PBHPC) not used in the original transplant.
• Mobilized PBHPC, although enriched for stem cells, still contain mostly lymphocytes
Collection
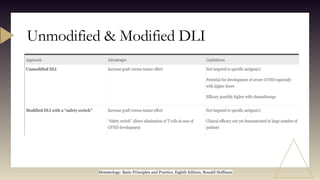
• Inserting asuicide gene in the donor T cells: If significant GVHD develops, T cells can be
turned off by activating this switch with a drug to avoid excessive GVHD.
• boost post-transplant immune recovery after T-cell-depleted haploidentical grafts
• Eg:
1)engineered T cells to express herpes simplex virus-thymidine kinase suicide gene that
can be targeted by ganciclovir to induce apoptosis.
2)engineered DLI to express an inducible caspase-9 transgene. This gene can be induced
by an inert dimerizing drug leading to rapid cell death
MODIFIED DLI
14.
Unmodified & ModifiedDLI
Hematology: Basic Principles and Practice, Eighth Edition, Ronald Hoffman
15.
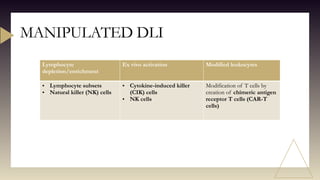
Lymphocyte
depletion/enrichment
Ex vivo activationModified leukocytes
• Lymphocyte subsets
• Natural killer (NK) cells
• Cytokine-induced killer
(CIK) cells
• NK cells
Modification of T cells by
creation of chimeric antigen
receptor T cells (CAR-T
cells)
MANIPULATED DLI
16.
Lymphocyte subsets –Fractionation of the donor product has been used to enrich CD4+ T cells or
deplete CD8+ T cells.
• Allogeneic HCT using alemtuzumab, DLI with CD8-depleted product accelerated immune
reconstitution, improved donor engraftment, and was not associated with significant GVHD.
• DLI with CD25/Treg-depleted product was capable of inducing GVT tumor responses without
excessive GVHD
Natural killer (NK) cells – NK cells exert potent GVT effects without initiating GVHD, and act
through a variety of cytokine receptors, and activating or inhibitory receptors.
• Alloreactive haploidentical NK cells can be safely administered and may reduce leukemia progression
without an increase in GVHD or transplantation-related mortality
Lymphocyte depletion/enrichment
17.
• Cytokine-induced killer(CIK) cells – Ex vivo culture of lymphocytes with interferon gamma, IL-2,
and anti-CD3 creates CIKs, which are cytotoxic T cells that recognize targets
• NK cells- ALT-803 is an engineered IL-15 superagonist complex which cause NK cell expansion and
activation with minimal changes in CD4+ T cells and Tregs. NK cells have also been used for
generation of CAR-NK cells with encouraging results
Ex-vivo activation
19.
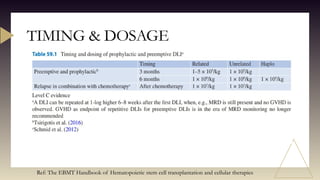
TIMING & DOSAGE
Ref:The EBMT Handbook of Hematopoietic stem cell transplantation and cellular therapies
20.
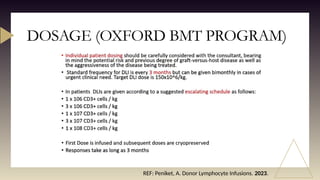
DOSAGE (OXFORD BMTPROGRAM)
REF: Peniket, A. Donor Lymphocyte Infusions. 2023.
21.
Factors that MayInfluence Timing, Dosing, and Frequency of DLI
• MRD: Six weekly scheduled DLI with escalating doses until the first signs of GVHD may not be
needed. A MRD-driven strategy with more time between DLIs (8–12 weeks) might still allow for
control of the hematological malignancy while avoiding long-term side effects like chronic GVHD. An
alternative is the infusion of donor αβT cells engineered with a suicide gene.
• Underlying disease: sensitivity is regarded as high for CML, myelofibrosis, and low-grade NHL;
intermediate for AML, MDS, multiple myeloma, and Hodgkin’s disease; and low for ALL and DLBCL.
• Combination with other drugs: Early administration of LENA after transplantation has been
associated with a high incidence of GVHD. Combinations with interferon-α and GM-CSF have also
been reported as successful intervention to enhance the GVL effect
22.
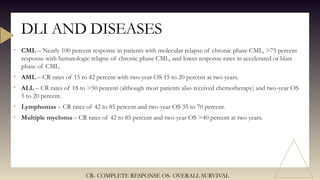
• CML –Nearly 100 percent response in patients with molecular relapse of chronic phase CML, >75 percent
response with hematologic relapse of chronic phase CML, and lower response rates in accelerated or blast
phase of CML.
• AML – CR rates of 15 to 42 percent with two-year OS 15 to 20 percent at two years.
• ALL – CR rates of 18 to >50 percent (although most patients also received chemotherapy) and two-year OS
5 to 20 percent.
• Lymphomas – CR rates of 42 to 85 percent and two-year OS 35 to 70 percent.
• Multiple myeloma – CR rates of 42 to 85 percent and two-year OS >40 percent at two years.
DLI AND DISEASES
CR- COMPLETE RESPONSE OS- OVERALL SURVIVAL
23.
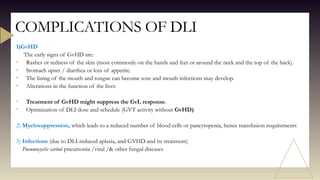
1)GvHD
The early signsof GvHD are:
• Rashes or redness of the skin (most commonly on the hands and feet or around the neck and the top of the back).
• Stomach upset / diarrhea or loss of appetite.
• The lining of the mouth and tongue can become sore and mouth infections may develop.
• Alterations in the function of the liver.
• Treatment of GvHD might suppress the GvL response.
• Optimization of DLI dose and schedule (GVT activity without GvHD)
2) Myelosuppression, which leads to a reduced number of blood cells or pancytopenia, hence transfusion requirements
3) Infections (due to DLI-induced aplasia, and GVHD and its treatment)
Pneumocystis carinii pneumonia /viral /& other fungal diseases
COMPLICATIONS OF DLI
24.
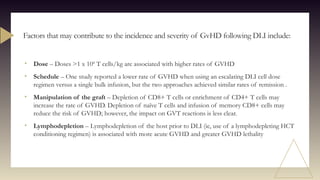
• Dose –Doses >1 x 108
T cells/kg are associated with higher rates of GVHD
• Schedule – One study reported a lower rate of GVHD when using an escalating DLI cell dose
regimen versus a single bulk infusion, but the two approaches achieved similar rates of remission .
• Manipulation of the graft – Depletion of CD8+ T cells or enrichment of CD4+ T cells may
increase the rate of GVHD. Depletion of naïve T cells and infusion of memory CD8+ cells may
reduce the risk of GVHD; however, the impact on GVT reactions is less clear.
• Lymphodepletion – Lymphodepletion of the host prior to DLI (ie, use of a lymphodepleting HCT
conditioning regimen) is associated with more acute GVHD and greater GVHD lethality
Factors that may contribute to the incidence and severity of GvHD following DLI include:
25.
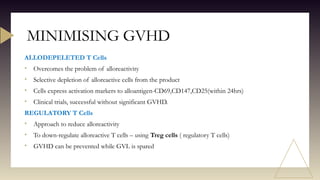
ALLODEPELETED T Cells
•Overcomes the problem of alloreactivity
• Selective depletion of alloreactive cells from the product
• Cells express activation markers to alloantigen-CD69,CD147,CD25(within 24hrs)
• Clinical trials, successful without significant GVHD.
REGULATORY T Cells
• Approach to reduce alloreactivity
• To down-regulate alloreactive T cells – using Treg cells ( regulatory T cells)
• GVHD can be prevented while GVL is spared
MINIMISING GVHD
26.
• Escalating DoseRegimen: lower rate of GVHD when using an escalating DLI cell dose regimen
versus a single bulk infusion, but the two approaches achieved similar rates of remission.
• Manipulation of the graft – Depletion of CD8+ T cells or enrichment of CD4+ T cells may
increase the rate of GVHD. Depletion of naïve T cells and infusion of memory CD8+ cells may
reduce the risk of GVHD; however, the impact on GVT reactions is less clear.
• Lymphodepletion – Lymphodepletion of the host prior to DLI (ie, use of a lymphodepleting HCT
conditioning regimen) is associated with more acute GVHD and greater GVHD lethality
• Use of irradiated lymphocytes in DLI
• Suicide genes - Herpes simplex thymidine kinase (HStk) gene, which is vulnerable to ganciclovir.
MINIMISING GVHD
27.
PRE-APHERESIS CHECKUP
Clinicalcheckup:
Medical history,
current medications,
physical examination,
and evaluation of
comorbidities
Venous access
assessment including
skin status
Complete blood count
Screening for
transfusion
transmissible
infections markers
Informed consent for
apheresis.
LEUKAPHERESIS/COLLECTION OF
LYMPHOCYTES
Performed on apheresis equipment to collect
lymphocytes.
Anticoagulant (acid citrate dextrose) is used
Monitoring of ionized calcium levels pre and
during procedure must be done
Procedure duration may be around 2–5 h.
Role of Transfusion Medicine
28.
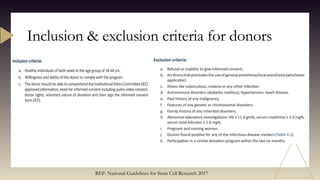
Inclusion & exclusioncriteria for donors
REF: National Guidelines for Stem Cell Research 2017
29.
• It ismandatory that the stem cells or their products/derivatives are processed in CDSCO licensed
Good Manufacturing Practices (GMP) compliant facility.
• Manipulated products: All laboratory procedures should be carried out under aseptic conditions in a
CDSCO certified GMP (schedule M) and GLP (schedule L 1) facility for human applications. For
preclinical studies on animals, the laboratory should have GLP certification from the Department of
Science and Technology (DST). Clinical application using such cells requires the IC-SCR, IEC and
CDSCO approvals.
• Clinical trials can be permitted only in institutions/hospitals having registered IC-SCR (with NAC-
SCRT) and IEC (with CDSCO).
Regulations
The National Apex Committee for Stem Cell Research and Therapy - NAC-SCRT
Institutional Committee for Stem Cell Research – IC-SCR
Central Drugs Standard Control Organization - CDSCO
30.
REFERENCE
• Parmar, S.;Ritchie, D. S. Allogeneic Transplantation as Anticancer
Immunotherapy. Current Opinion in Immunology 2014, 27, 38–45.
https://doi.org/10.1016/j.coi.2014.01.010.
• The EBMT Handbook of Hematopoietic stem cell transplantation and cellular
therapies
• Peniket, A. Donor Lymphocyte Infusions. 2023.
• Negrin, R. S. Immunotherapy for the Prevention and Treatment of Relapse
Following Allogeneic Hematopoietic Cell Transplantation.
• Hematology: Basic Principles and Practice, Eighth Edition, Ronald Hoffman
• National Guidelines of stem cell research, 2017







































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















